This story is the first in a series covering personal-care products that are harmful to well-being and the environment.
ANYONE WHO’S environmentally consciousis very concerned about microbeads, those tiny spheres of plastics that range in size from a pinhead to as small as one micrometer. That’s despite the Microbead-Free Waters Act of 2015 that former President Obama signed into law, phasing out microbeads in “rinse-off” products and toothpaste by late 2017. The new law fails to cover cosmetic creams, deodorants and make-up, in particular “age-defying” wrinkle creams, as well as household cleansers. Also, bead-laced formulations already purchased by those who tend to stockpile languish in medicine cabinets and travel bags.
Microbeads can cause harm when toothpaste microbeads get “stuck in the tiny crevices between the teeth and gums,” according to a Washington Post article, which goes on to quote Phoenix, Arizona, dentist Justin Phillip: “They’ll trap bacteria in the gums, which leads to gingivitis, and over time that infection moves from the gum into the bone that holds your teeth, and that becomes periodontal disease.”
According to The Post, both the FDA and the American Dental Association have firmly supported the safety of microbeads. But the makers of Crest, admitting that the beads’ sole raison d’etre in toothpaste is color and sparkle, promised to phase out microbeads completely by March 2016.
Microbeads are a menace to the environment. Too tiny to be filtered out by wastewater treatment plants, the beads proceed to clog rivers, lakes and the ocean. They absorb polluting chemicals, are consumed by fish and can harm both the fish and anyone who eats them. A single cleansing product can contain up to 360,000 microbeads, according to The Guardian.
One estimate says Americans flush billions of microbeads down the drain every day. Microplastics found in the world’s water also come from clothing fibers, boat paint and degrading plastic bags and bottles.
The best microbead substitute is sand: one cosmetic company has created “synthetic amorphous silica” with claims of “higher purity” than the beach. Exfoliants on the market for years have used pumice, jojobeads, apricot kernels, ground nutshells—even salt and sugar.
The International Campaign Against Microbeads in Cosmetics has a list of microbead-containing products—including those with such healthy-sounding names as Aveeno “Active Naturals.” To be sure, check ingredient labels for the most common plastic components of microbeads: polyethylene (PE), polypropylene (PP), polyethylene terephthalate (PET), polymethyl methacrylate (PMMA), polytetrafluoroethylene (PTFE) polylactic acid and nylon.
Or use the free Beat the Bead smartphone app that scans a product’s barcode for plastics. Among good-guy/-gal cosmetic manufacturers using no microplastics are L’Oreal, Clarins, Botanicals and Clorox (Burt’s Bees), along with many others listed by the story in The Guardian.
What you can do with microbead-containing products still on hand is donate them for research* or ship them back to the manufacturer. ** For the very energetic, there’s a cumbersome DIY filtering process, although it’s not clear that those microbeads end up in a better place. Although clearing plastics out of the ecosystem might be impossible, the best hope for the future is that the burgeoning field of “green chemistry” can better investigate new products before more damage is done.
*The 5Gyres Institute, 3131 Olympia Boulevard, Santa Monica, California 90404; or Sherri Mason, SUNY Fredonia, 280 Central Avenue, 340 Sciences Complex, Fredonia, New York 14063.
**The International Campaign Against Microbeads in Cosmetics has a sample letter to send with the returned product.
Voltaren: The Best Pain Relief You’ve Never Heard Of
iStock
FOR THE FASTEST and safest relief for pain, particularly that caused by osteoarthritis, many turn to Voltaren. Don’t know it? That’s because in the U.S. this ibuprofen-like gel is unavailable without a prescription. Having a tube on hand to try before or instead of seeking medical attention requires planning ahead, importuning your doctor for a Voltaren Rx just in case.
Alternatively, you can buy a few tubes—around $10 each—when traveling to another country like Canada, although take care when returning through Customs. Some Canadian pharmacies handle prescriptions online, although shipping costs add up, and this route can be unreliable as well as illegal. The FDA web site warns: “Don’t purchase from foreign web sites at this time because generally it will be illegal,” the word generally inspiring both guffaws and online orders.
Voltaren is diclofenac, an NSAID (non-steroidal anti-inflammatory drug) that blocks the immune system’s inflammatory response to injury, pain and stress on bones, joints and muscles. (Voltaren also comes as a patch to treat acute pain of strains, sprains and bruises, though obtaining these is also complicated.) Topical NSAIDs work best for short-term use, under four weeks.
Of four kinds of OTC pain medication, acetaminophen (Tylenol) is good for treating fever and most pain but less effective for musculoskeletal pain, and risks liver damage compared to the others: aspirin, ibuprofen and naproxen (Aleve). These three NSAIDs treat inflammation as well as pain and fever, but can risk irritating the GI tract, especially aspirin.
Rather than a “gut burner,” Voltaren gel can (for about 5% of patients) be a “skin burner,” causing redness at the site of application. By reducing exposure to the rest of the body, however, topical NSAIDS lower the risks of serious side effects, in particular those related to blood clotting.
Popular topical treatments, including salicylates (BenGay, Aspercreme) and capsaicin, along with the homeopathic Arnica montana (Traumeel), “have shown little potential in the past,” according to Paul Ingraham, creator of PainScience.com. Ingraham can buy Voltaren gel from “a rack of tubes…by the till at my neighborhood drugstore” in Vancouver.
Pain-killing gel, he explains, is most helpful for “accessible” joints, those not covered by a thick layer of muscle (like the shoulder), because “the medication gets diluted as it penetrates deeper into tissue.” Among conditions that gel can help: plantar fasciitis, shin splints, tendinitis where the tendon is just under the skin—in the elbow, Achilles, knees and fingers (carpal tunnel syndrome)—strains and bursitis.
“Surprisingly, Voltaren may even help some kinds of deep back pain,” Ingraham writes. In most cases, however, topicals don’t work well for deep tissue pain like muscle soreness, nor for conditions causing little or no inflammation. With repetitive strain injuries like tendinitis, there can be some inflammation, but “the chemistry is complex,” explains Ingraham. Generally, muscle pain in the low back, the neck and deeper in the body is unrelated to inflammation and thus unresponsive to topical gels.
In a Cochrane “systematic review” of current literature (61 studies, 8386 patients) that looked at patient improvement around 7 days after the injury—the accepted wisdom being that after that time most get better without treatment—diclofenac gel reduced pain for 7 or 8 of 10 patients, compared with 2 to 3 out of 10 with a placebo.
In the review, gel formulations of diclofenac, ibuprofen and ketoprofen, and some diclofenac patches provided the best effects for “painful strain, sprain or muscle pull.” About one in 20 had redness at the application site.
While U.S. residents await OTC Voltaren gel, researchers at the University of Warwick (England) have created an ibuprofen patch that can deliver a consistent high dose at a steady rate over about 12 hours. According to early results, this patch “opens the way for development of a range of novel long-acting, over-the-counter pain relief products” to treat common painful conditions without the side-effects of oral drugs, according to Science Daily.
Marketing of the new patch is expected to begin by the end of 2017. The question remains, however, about how many additional years U.S. residents will be obliged to wait—and could inspire future travel plans to Canada.
—Mary Carpenter Mary Carpenter is the well-being editor of MyLittleBird. Read more of her posts here.
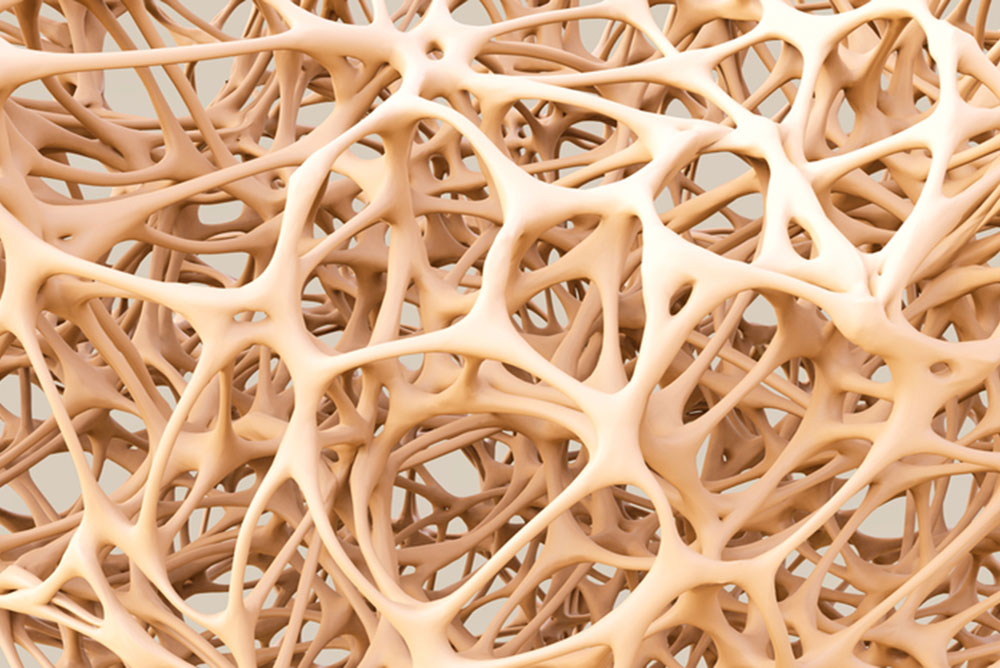
DISCOVERING THAT the same drug targeted at halting osteoporosis—with its increased risk of broken bones—can over time cause those same bones to break serves as a warning: wait before starting a newly approved drug—for 10 years or longer if possible. Consider the case of osteoporosis drug Fosamax.
Since its introduction in 1995, Fosamax has been snowballing side effects, many resulting in warnings from the FDA. The biggest risk appears to be “low-energy” or “stress” fractures” to the thighbone. Femur fractures can occur as a result of low-impact force—a fall from standing height or less—or sometimes as little as turning the body the wrong way, stopping the car suddenly or simply walking.
The bisphosphate Fosamax works to increase bone density by slowing the body’s natural process of bone breakdown and resorption. It was the first drug on the market to slow bone loss, which can lead to crippling fractures of the hip and spine.
How the drug causes femur fractures is still unclear. It kills cells designed to remove old bone, with the result that there might be too little room for new bone growth. The drug could also interfere with the repair of microscopic cracks caused by normal wear and tear, and then microdamage accumulates over time to cause fractures.
Or Fosamax could cause bones to become more brittle and thus less resistant to wear and tear, perhaps in the process of slowing bone turnover or as it suppresses bone breakdown with ongoing mineralization of the bone. Finally, the active ingredient in Fosamax, alendronate, may slow the development of new collagen, found in abundance in bones.
In the drug’s first year, the FDA warned the manufacturer Merck of overstating its benefits and minimizing its risks. Within several years of approval came the first reports of femur fracture. But not until 2008 did a study in Singapore report on 17 women—average age of 66, average length of time on Fosamax of five years—who had femur fractures without major trauma. Of these, 13 had leg pain before the fracture occurred.
A subsequent study at New York’s Hospital for Special Surgery, found that of 25 patients taking Fosamax, 20 had a femur fracture and 19 of these occurred in patients taking Fosamax the longest. More problems arose when physicians began prescribing Fosamax for osteopenia, a slight thinning of the bones that can precede osteoporosis—which previously had been untreated, and which many physicians consider insufficiently worrisome to require any treatment at all (see MyLittleBird story on osteopenia).
While a 2008 Harvard Health Letter concluded that “most experts believe that when Fosamax is used appropriately, its benefits greatly outweigh the risks,” by 2014 the Harvard Letter suggested that most women should consider taking a “bisphosphonate drug holiday” after three to five years.
Meanwhile as early as 2004, Fosamax was linked to “Dead Jaw Syndrome” (osteonecrosis of the jaw) that can eventually cause the jawbone to collapse completely. Although the cause is still being investigated, patients are urged to consider having dental surgery before starting Fosamax—that is, when such surgery can be anticipated. Fosamax-related lawsuits against Merck were filed beginning in 2004.
In 2008, the drug was linked to esophageal cancer. In addition, Foxamax has caused burning in the esophagus as well as “incapacitating bone, joint and muscle pain,” according to the Drugwatch.com report.
In 2010, the FDA required labels warning about the risk of thighbone fractures. Currently, an FDA advisory committee wants to limit the amount of time a patient takes Fosamax but has not yet come up with a specific limit. In addition, the WHO has developed a scale to help determine which osteopenia patients might benefit from the drug.
Because it takes about 10 years for bisphosphonates stored in the body to decline by half, the recommendation for those taking a “drug holiday” is to test bone health every two years after stopping the drug. In one study, women who had taken Fosamax for at least five years were divided into two groups, one continuing the drug and the other taking a placebo. After five years of the study, the rate of hip fractures—considered “a far more serious injury” compared to fractures of the spine or femur—was the same for both groups.
On the other hand, those at highest risk of hip fracture—those who’ve had a fracture in the past and had low bone density when starting therapy—might benefit more from continuing the drug compared to the risks of a drug holiday. But try telling that to someone who has suffered a femur break—unexpected, with little provocation—after taking Fosamax: most of these women want nothing more to do with the drug.
THE FDA, THE CDC and the FCC have all concluded that there is no scientific evidence supporting the risk of brain cancer from cell phone use. But for those worried about the risks of radiation—both from cell phones themselves and possibly from Bluetooth earpieces as well—the recommendation is to use cell phones on speaker.
Fears about cell phone dangers are fanned on sites like cellphonecancer, created by personal injury attorneys Frasier, Frasier & Hickman, LLP. And by Devra Davis, director of the University of Pittsburgh’s Center for Environmental Oncology, whose warnings sound overblown when she calls cell phone dangers “the most important and unrecognized public health issues of our time,” and says, “We could avert a global catastrophe if we act.”
But in his review of Davis’s book, “Disconnect,” Time magazine science writer Bryan Walsh writes: “Davis makes a strong case…that we’ve underplayed the possible threat from cell phones for too long. As Davis points out, most studies that find no evidence of dangers from cell phone radiation are funded by the cell phone industry, while dangers at more than twice the rate have been found in independent studies.
“The fact that we don’t know everything about the subject doesn’t mean that everything is fine,” Davis says. “I can’t tell you that cell phones are dangerous, but I can tell you that I’m not sure they’re safe.”
After the most recent animal studies—by what she calls the U.S. government’s “premier” National Toxicology Program–Davis wrote, “We now have three different studies within the past six years where animals develop some of the same cancers from cell phone radiation as people…unusual highly malignant brain tumors—gliomas—as well as very rare tumors of the nerves around and within the heart.” She notes that the gliomas occurred only in male rats.
The sole biological effect of electromagnetic radiation—used by cell phones, TVs and radio transmissions and microwaves—is heating. This non-ionizing radiation has lower energy or power frequencies compared to ionizing radiation, for example, of x-rays. Using cell phones can slightly heat the ear or head but not enough to measurably increase body temperature. Also, concerns that radiofrequency energy might affect glucose metabolism or blood flow in the brain remain unsupported by the research, according to the National Cancer Institute.
Those asserting the safety of cell phones point to an NCI data analysis of the incidence of brain or other nervous system cancers between 1992 and 2006, when cell phone use exploded, which detected no increase. (The risk of developing brain cancer does, however, increase with age: from 2008 through 2012 in the U.S., there were approximately 19 cases for every 100,000 people ages 65 and older, compared to fewer than five per 100,000 under age 65.)
When a WHO working group in 2011 classified cell phone use as “possibly carcinogenic to humans,” the American Cancer Society explained that classification as meaning there “could be some cancer risk associated with radiofrequency energy but the evidence is not strong enough to be considered causal.”
Those most likely to be affected by cell phone risks are the “heaviest” users. Doubts about cell phone safety were raised, also in 2011, by two Swedish studies that reported increased brain cancer risk—based both on total amount of cell phone use and on years of use among people who began using cell phones before age 20.
A multicenter study in France from 2004 to 2006 that showed no association of risk when comparing regular cell phone users with non-users did find “significantly increased risk” of both gliomas and meningiomas among the heaviest users. In addition, incidence data from Denmark, Finland, Norway and Sweden for 1974-2008 could not rule out increased risk among the heaviest cell phone users.
“Interphone,” one of the three largest epidemiological studies, conducted by researchers in 13 countries, found a modest increase in risk of gliomas among the small proportion of study participants who spent the most time on cell phone calls—although the finding was considered inconclusive. Another analysis from this study found no relationship between brain tumor locations and regions of the brain exposed to the highest level of radiofrequency energy from cell phones.
Two studies sponsored by the National Cancer Institute in multiple U.S. academic medical centers between 1994 and 1998 showed no relationship between cell phone use and increased risk of cancer. And an international study of children diagnosed with brain cancer between ages 7 and 19 found no relationship to cell phone use.
Many difficulties that plague research on the connection between cell phone use and brain cancer can cause these discrepancies. “Recall bias” occurs when memories of those diagnosed with brain tumors are altered by simply getting the diagnosis and/or by the physiological effects of tumors, compared with those who suffer no ill effects. Inaccurate reporting occurs in all retrospective studies, as does “participation bias”—in this case, that people with tumors are more likely to enroll in studies.
Although the FDA takes the position that research showing any ill effects have failed to be replicated and epidemiologic studies have failed to document a relationship, it does suggest using hands-free technology when possible. According to the NCI site, “exposures decline dramatically when cell phones are used hands-free.”
The worriers agree. Every inch away from your body, the radiation reduces very quickly, explains Magda Havas at Ontario’s Trent University: “Hold it out two inches, and the radiation drops by a factor of four.” She suggests holding the phone a minimum of a few inches away— but “a foot or two is ideal.”
The FDA’s other suggestion: “Reserve the use of cell phones for shorter conversations or for times when a landline phone is not available”—that is, if you still have access to such a thing.
—Mary Carpenter Mary Carpenter is the well-being editor of MyLittle Bird. Read more of her posts here.
WHEN SOMEONE remarked that I seemed to be dragging my left foot, I had no idea—not why it started or how long it had been that way or even that I was doing it.
Everyone’s body is unbalanced—not wobbling when you stand on one foot, but having one side stronger or more stressed or more painful than the other. Starting before birth, the fetus curls in one direction. Next come years with the right side heavier—because of the liver, around three pounds for a woman—than the left, which has only the heart, at little more than half a pound, helped by the stomach but only when full.
Daily activities that unequally stress the dominant side include eating, writing, carrying a purse, playing almost any sport. To drive a car, your right side always gets in first, and your right foot usually does most of the work. One side gets into bed first.
Using a computer mouse with your right hand if it’s the dominant one, “your right pectoral (chest) muscle will become shorter,” writes Todd Kuslikis on A Shot of Adrenaline. “At the same time, the muscles on the right side of your back will elongate and rotate the portion of the spine they are linked to. This causes some interior spinal muscles to become atrophied, potentially causing pain by pinching nerves.”
Imbalance is exacerbated by injury. And after the injury heals, favoring one side has become so automatic that the body keeps performing off-kilter. Internal surgery, such as an appendectomy or a C-section, leaves scar tissue that pulls in one direction or the other.
To assess imbalance, look in the mirror—especially at the hips and shoulders. If one shoulder is higher or lower than the other, you’ll be strengthening and/or pinching one side, writes Greg Presto on Shape.com.
For those with chronic pain in joints and muscles, “repetitive movement is the culprit…crowds out the full range of spontaneous movement upon which the body depends for total function,” writes Pete Egoscue in “Pain Free for Women.”
“Disengaged muscles and a misaligned skeleton can take the edge off any fitness and exercise routine…why most people don’t stick with them,” according to Egoscue. “Over time, neglected muscles and structures get harder to move.”
Before starting strength training, the musculoskeletal system (MS) should be operating correctly for at least a month, he contends. And correcting imbalance can alleviate chronic pain and make weight loss easier. Chronic MS pain, Egoscue writes “is symptomatic not of advancing and accumulating years but of advancing and accumulating dysfunctions.”
The “Egoscue Method,” available locally at personal fitness specialists Dave Reynolds and Associates in Silver Spring, claims to “help thousands of individuals tap into their body’s ability to heal itself and free themselves of chronic pain.” An Egoscue therapist begins by assessing your basic structural alignment, in addition to conducting a lengthy interview about injuries, weaknesses and general health. An individualized program of “E-cises” (E for Egoscue) is created to correct imbalances and built on as you progress.
General advice for rebalancing your body: start workouts with the weaker side, and let that side’s performance determine what the other side does in terms of weights and repetitions—and/or do extra work on the weak side. While walking, biking, swimming, I make my left leg and foot work harder, when I remember.
The best exercises are isometric: holding a static position against a fixed resistance, often a wall—for at least 30 seconds. To stabilize and rebalance shoulders, stand with forearms pressing against a wall. For the legs, lie on your back with your legs bent and feet pushing against the wall.
Good exercises for the upper body include planks, push-ups and squeezing a large ball between two hands; for the lower body, squats with your back against a wall, lunges and a hip lift or bridge.
For isometric exercises, don’t hold your breath—for two reasons. Literally, because these exercises can cause blood pressure to rise. And figuratively, because benefits in improved balance and tone from isometric exercises occur very slowly over time.
IT HAPPENED to a 66-year old woman, known in her workout classes as the “cardio queen” for exerting herself more strenuously than the others. And to a 52-year old man who has participated in sprint- and Olympic-distance marathons, working up to the half-Ironman. Both began fainting suddenly, and then both had pacemakers implanted in their hearts.
Serious aerobic and endurance exercise, while good for the heart, can over time cause the heart rate to drop below 30 beats/minute, called bradycardia—compared to a typical healthy resting heart rate of 60-100 BPM. A very fit individual’s heart has a larger stroke volume—meaning that each heartbeat delivers more oxygen to the heart—so the resting heart can beat more slowly.
Research on rodents has shown that endurance exercise training causes molecular changes in the heart’s pacemaker (rather than changes in the autonomic nervous system, which was previously assumed). These changes “may help us to understand the more frequent occurrence of heart rhythm disturbances or even loss of consciousness in athletes,” said one of the study’s researchers, based at the University of Manchester in England.
“Elderly athletes with a lifelong training history are more likely to need an artificial electronic pacemaker,” the study’s lead researcher said. (Because the study dealt with rodents, what he had in mind by “elderly” wasn’t clear.)
Of two kinds of exercise, endurance training involves sustained elevation of heart output, while strength training involves short bursts of intense heart contractions. Some sports like cycling combine both: more than half of 286 Tour de France cyclists (from 1995 and 1998) had abnormally low resting heart rates—measured as ejection fractions, the percent of blood ejected from the heart at each beat.
Fainting has several causes, and only the most common—called cardioinhibitory syncope, with syncope meaning loss of consciousness—is relieved by implanting a pacemaker. It can occur when the heart rate slows to less than 40 beats per minute with a resulting drop in blood pressure. With another cause called vasovagal syncope, falling blood pressure is the instigator, the result of blood vessels failing to get the blood flowing back up to the heart, so that blood pools in the legs. The third cause is a combination of the two.
What’s important is identifying the primary cause—slow heart rate or low blood pressure—which can be determined by a tilt table test: when the head is elevated above the feet, heartbeats should increase to pump more blood to the head: when that doesn’t happen, it means the heart could use some help, such as from a pacemaker, to work more efficiently.
For some with cardioinhibitory syncope, the heart can stop completely—called asystole. A dual-chamber pacemaker detects a heart rate falling below 40 BPM, or an abrupt drop of 20 BPM, and paces the heart at a faster rate for a fixed period of time. In one study, pacemakers reduced fainting episodes by more than 50% in those who had experienced asystole lasting six seconds or more.
While fainting can be dangerous, merely feeling faint or lightheaded (called presyncope) might not be a good reason for a pacemaker. A man in his 70s who was scheduled for pacemaker surgery sought a second opinion only to learn that the low heart rate causing his faintness was due at least in part to medication he was taking for a different heart problem. Switching medications eased the problem.
Skeptics, including some cardiologists, think pacemakers are prescribed too readily because physicians don’t want to be responsible for dangerous fainting episodes. Others point out that pacemakers provide an income stream because the devices must be checked every six months.
But the first randomized controlled study of pacemakers for vasovagal syncope, published in 1999, was terminated early because of the “vastly significant success” of pacemaker trials in the first 54 patients, each of whom had suffered more than six episodes of fainting. Although mild lightheadedness persisted even in those who received pacemakers, their chances of recurrent episodes were reduced 85%.
—Mary Carpenter Read more posts from Well-Being EditorMary Carpenter.
IN THE CATEGORY of what to watch out for in fish oil supplements, mercury, lead and PCBS have gotten attention. But those alarms appear to have been overblown. More worrisome concerns with supplements, however, are mislabeling as well as 15 specific ingredients found in products sold everywhere—including CVS and Whole Foods, according to a list published by Consumer Reports in July, 2016 (see list below).
First, about fish oils. Testing by ConsumerLab.com of omega-3 supplements found “none to contain mercury and most to have only trace levels of PCBs (which can’t be fully avoided since PCBs are found in water everywhere).” The conclusion: “A serving of fish is likely to contain far more contamination than supplements.”
On the other hand, ConsumerLab’s testing found that mislabeling affected “at least a third of the supplements tested. One of the products had only half the amount of DHA [along with EPA, promoted for brain and heart health], and another contained only two thirds.”
Additional testing by LabDoor of 30 top-selling fish oil supplements found that six of the products had 30% less omega-3s than listed on the packaging, and at least a dozen products had levels of DHA 14% below that listed on the packaging.
“I wouldn’t advise any fish oil pills that aren’t molecularly distilled, and I usually recommend Nordic Naturals,” notes Susan Allport, journalist and author of “Queen of Fats: Why Omega-3s Were Removed from the Western Diet and What We Can Do to Replace Them.” She adds, however, that “nutrients including omega-3s, are usually absorbed better through foods than [through] supplements.”
Risks of the 15 ingredients listed by Consumer Reports (CR), on the other hand, include organ damage, cancer and cardiac arrest. Many interact with medications such as statins and blood-thinning drugs, including aspirin. The “severity of these threats often depends on such factors as pre-existing medical conditions as well as the quantity of the ingredient taken and the length of time a person has been exposed to the substance,” according to the report.
In addition, “none of these supplement ingredients provides sufficient health benefits to justify the risk,” according to the experts assembled by CR.
Supplements are sold with no official monitoring or regulating. Between 2008 and 2011, the FDA received reports of more than 1,000 serious injuries or illnesses and 92 deaths due to dietary supplements.
“Because of the way they’re regulated you often have no idea what you’re actually ingesting,” notes Pieter Cohen, assistant professor at Harvard Medical School. Cohen recently won a defamation suit brought against him by Hi-Tech Pharmaceuticals—makers, for example, of Black Widow and Yellow Scorpion taken for weight loss—for criticizing that company’s supplements, some of which are still on the market.
The 15 risky Consumer Reports ingredients can be divided into groups for easier recall based on alleged benefits. First, the five widely used by women—those not primarily for weight loss or respiratory issues—include aconite (inflammation and joint pain); caffeine powder (attention); kava (anxiety and insomnia); red yeast rice (cholesterol), and celandine (stomachache).
For weight loss: chaparral, germander, green tea extract, methylsynephrine and usnic acid. And the rest: coltsfoot (cough, sore throat); comfrey (cough, also heavy menstrual periods); pennyroyal oil (breathing problems), and lobelia (respiratory problems). No. 15 is yohimbe for erectile dysfunction and low libido, also depression and obesity.
Over the years, some harmful supplement ingredients have been eliminated, notably anabolic steroids once found in supplements sold by a vitamin company that’s still in business, according to “If Our Bodies Could Talk,” by James Hamblin.
News reports, however, continue to warn about worrisome products. In the first month of 2017, the New York Times reported on a study (published in the November Journal of Clinical Sleep Medicine) finding “71 percent of melatonin samples were more than 10% off the stated dose, with some lots containing nearly five times the listed dose.” Another survey found the Ubervita brand contained .01 mg of melatonin, 99.8% below the label claim.
The advice is to buy only “pharmaceutical grade” melatonin—including brands such as “Just Potent,” recommended by the American Sleep Association. And for any supplement, do research before selecting the brand—go beyond just checking for best sellers and low prices on Amazon.
Greater Celandine
Also called: Celandine, chelidonium majus, chelidonii herba
Alleviates stomachache
Liver damage
Green Tea Extract Powder
Also called: Camellia sinensis
Weight loss
Dizziness, ringing in the ears, reduced absorption of iron; exacerbates anemia and glaucoma; elevates blood pressure and heart rate; liver damage; possibly death
Kava
Also called: Ava pepper, kava kava, piper methysticum
Reduces anxiety, improves insomnia
Liver damage, exacerbates Parkinson’s and depression, impairs driving, possibly death
ALTHOUGH THE PLANET is warming with every passing year, temperatures around the DMV can fluctuate so wildly over a period of hours that it’s never safe to forget entirely about frostbite. Go for a walk or bike ride, and the trip home can become suddenly and worrisomely cold, windy and wet.
Loss of sensation in fingers, toes, ears and noses calls for taking correct measures and avoiding wrong ones. Among the latter: hot water, dry heat such as fire, rubbing and walking on affected toes.
Most important: If there’s any chance of refreezing in the immediate future, nothing at all should be done. Fluids within frostbitten tissue can form ice crystals, causing potentially permanent changes in the cells. Refreezing delicate frostbitten tissue creates greater risk of the worst outcomes, including gangrene and amputation.
Frostbite is more likely with exposure to below-freezing temperatures, especially with high winds and wet conditions, and with unsuitable clothing — either too tight or not protective against cold, windy or wet weather. To preserve body temperature, blood vessels close to the skin surface constrict, and blood is shunted away from the extremities.
Metal jewelry can speed cooling, and ears are among the most often frostbitten body parts. Besides weather, other causes of frostbite include touching ice, cold packs or frozen metal; and prolonged exposure to aerosol sprays, for example, causing deodorant burn.
Risk increases for both infants and older people; and with dehydration, exhaustion and medications like beta-blockers. And because of anything that limits blood flow to the extremities, including poor circulation — for medical reasons, or because clothes or boots are too tight — and peripheral neuropathy, alcohol and nicotine, heart disease and diabetes. Also: fear or panic, previous frostbite or cold injury, and high altitudes, which reduce oxygen supply to the skin.
In very cold weather, the body’s first reaction is “frostnip,” with skin turning pale or red — followed by red, white or yellow patches, itching, pain and prickling. Also, numbness that can prevent recognition of problems until someone else points them out. Superficial or second-degree frostbite comes next, causing the skin to turn paler, harden and begin to feel warm — the last is an especially bad sign. Warming the area at this point may cause stinging, burning and swelling; skin appearing mottled, blue or purple; and blisters appearing within 36 hours.
Severe, third- and fourth-degree, deep frostbite causes the skin to feel hard and waxy with loss of all feeling of cold or discomfort, and large blisters that form in the first 48 hours. The blisters are purple but turn black, and are usually filled with blood. Pain, skin that remains red or pale, blisters and fever all indicate the need for medical attention.
(Chilblains, also called perniosis, is a different reaction to cold in predisposed individuals, in which capillaries close to the skin surface are damaged, causing redness, itching, inflammation and sometimes blisters.)
For any stage of frostbite, the best first response is to soak the affected body parts in water that is warm — not hot but comfortable to the touch — and leave them there for 30 minutes, which can be painful enough to require OTC painkillers. Seriously frostbitten extremities should be elevated and wrapped or splinted to prevent any ice crystals from moving around, which can cause further damage. Drinking hot liquids like tea or hot chocolate can help as can exercise to keep the blood flowing — but only if the condition is mild and with care to avoid exhaustion.
When stranded in a car, make sure the exhaust pipe is cleared of any snow or ice, the engine and heater can be run for ten minutes every hour, with one window slightly open to avoid carbon monoxide fumes.
The best prevention is loose-fitting layered clothing, with inner layers of wool, silk or polypropylene; and wind-resistant outer layers to avoid losing body heat in cold wind, according to the CDC. Also, despite their renowned unreliability, keeping track of weather reports is a good idea.
The best defense, of course, is the coming of spring. With the December 21 solstice finally past, the days are getting longer, and warm weather is around the corner — in three months or so.
— Mary Carpenter Mary Carpenter is the well-being editor of MyLittleBird. Click here to see more posts.
TO TAKE ADVANTAGE of currently legal marijuana-infused lotions, or “topicals”— with benefits from reducing inflammation, pain and itchy skin to amplifying sexual pleasure — you might want to visit a “medical marijuana state” like California or Colorado before Donald Trump’s administration gets to work. Or in the DMV, with varying degrees of legality, you can make your own.
While many states allow sales of some formulations of marijuana oil — in stores and online, but not to be sent or transported back to “prohibitionist” states — the federal CSA (Controlled Substances Act) still deems all marijuana illegal. And although President-elect Donald Trump appears to support medical marijuana “100 percent,” his proposed attorney general, Alabama senator Jeff Sessions, has said repeatedly that “this drug is dangerous.”
Writes Politico reporter James Higdon, “With little more than the stroke of his own pen, the new attorney general will be able to arrest growers, retailers and users, defying the will of more than half the nation’s voters.” Post-2016 elections, the U.S. has 28 “medical states” plus D.C.; and 14 additional states have approved marijuana-infused topicals, also referred to as CBD-oil.
Marijuana topicals are divided into categories depending on each state’s regulations and on the percent of tetrahydrocannabinol (THC), the only identified psycho-active and otherwise potentially most medically active of some 80 cannabinoids contained in marijuana. When applied in topicals, THC binds to endocannabinoid receptors beneath the skin but doesn’t enter the bloodstream, thus causing no psycho-active effects (unless administered via transdermal patch).
In marijuana topicals, the most active ingredient is another cannabinoid called CBD cannabidiol (CBD), though many contend CBD merely softens the skin without the addition of enough THC to enhance medicinal effects, including reducing inflammation and pain, especially that related to arthritis, tendonitis, fibromyalgia and neuropathy; relaxing muscles; and speeding wound-healing. Because the skin has a low absorption rate for cannabinoids, the recommendation for most topicals is to apply “liberally” to the affected location.
While hemp and marijuana are members of the same plant species, Cannabis Sativa L, hemp is grown around the world for food, oil and fiber and naturally has almost no THC. CBD oil obtained from hemp products contains less than 0.3 % THC and is legal in most states. (Concentrations of THC in marijuana range from 0-35%.)
But most agree that marijuana extracts containing more THC work better. Vogue editor Eviana Hartman “swears by Apothecanna’s minty, cooling Extra Strength Relieving Body Crème…for lower-back stiffness.”
Among cannabis topicals for the bedroom, Pleasure oil from Foria, prescribed by at least one L.A. based sexual-health clinician, comes with claims that “when applied externally and internally [it] increases blood pressure and nerve sensation.” Directions for Foria Pleasure begin: “apply 4-8 sprays directly onto the clitoris, inner and outer labia and inside the vagina” and “allow 15-30 minutes to relax and absorb the medicine.” One customer touts its advantages as a lubricant that’s not messy like K-Y jelly.
Cannabis Basics CEO Ah Warner explains that each topical preparation has unique healing properties: the cooling THC-rich rub can help wind down from a workout, while a warming balm combines painkilling properties with a soothing sensation. “Cannabusinesses,” such as Kush, Cannabis Basics and Mary’s Medicinals —especially those that are home-based — have enabled more women to enter the traditionally male-dominated world of retail marijuana.
Unfortunately, federal regulations place all topicals containing more than .3% THC with marijuana under the Schedule I drug classification — alongside heroin, LSD and ecstasy — as having no currently accepted medical use and high potential for abuse. Even cocaine and meth, as Schedule II drugs, are under fewer restrictions. As long as federal prohibitions exist, physicians may recommend but cannot prescribe marijuana, and anyone possessing it anywhere in the U.S. risks prosecution.
For medical, recreational and merely decriminalized marijuana, each state has different, often very specific regulations. Among those that approve CBD-oil for medical use, for example, Florida allows no more than .8% THC.
Both D.C. and Maryland allow medical marijuana, including CBD-oil, with recommendations from certified physicians — along with, in Maryland, a state-issued medical marijuana card, and in D.C., registration with the mayor’s office. Virginia has passed a bill allowing the production and distribution of two marijuana-based oils but is awaiting regulations to be created by the state board of pharmacy.
While Jeff Sessions and others criticize all marijuana users, surveys have shown that of medical cannabis card-holders, 85% have some form of higher education, 45% have children, most have good jobs and most are in their 40s and 50s. In California, half of card-holders report using marijuana to treat pain, anxiety, cancer, seizures and auto-immune conditions — as a substitute for prescription drugs and specifically for opiates currently contributing to an epidemic of abuse.
For DIYers, creating marijuana topicals — to use alone or mix into customary lotions — according to recipes available online, requires just a few steps: baking the marijuana in a low oven for 45 minutes (called decarboxylating); adding it to an oil base, such as coconut, almond or grapeseed; simmering the mixture in a double boiler for 30 minutes or so; straining and cooling. Warning: except possibly in D.C. where residents are allowed up to two ounces of marijuana each for personal use, possession of such home-made topicals may be illegal.
— Mary Carpenter Click here for more of our Well-Being editor’s posts.
AH, DEPRESSION, always good for a sad holiday topic. But there are other approaches, such as why almost everyone these days seems to be taking an anti-depressant. Or, the role of antibiotics and other drugs in contributing to depression.
But the best may be a recent study focusing on “the bright side of being blue” — the actual title of a research paper touting “analytical rumination — a type of distraction-resistant thinking that is characteristic of depression.
(Note: Analytic rumination, holiday blues and whatever is being treated in people who function well on anti-depressants are all a far cry from the acute or chronic depression that cripples its sufferers.)
The startling rise in anti-depressant use — from almost 7% of Americans in 1999 to about 13% in 2012, according to statistics from the NHANES (National Health and Nutrition Examination Survey) of 37,959 adults over age 20 — is causing an outcry by some but not all of the medical profession.
Among women in their 40s and 50s, one in four now takes an antidepressant medication, according to a Johns Hopkins study on more than 5,000 patients who had received a diagnosis of depression within the previous 12 months. The study’s conclusion, which criticized overprescription of the drugs: two thirds of the 5,000 did not meet the criteria for “major depressive episode” as described by the Diagnostic and Statistical Manual of Mental Disorders (DSM), the New York Times reported.
On the other hand, “Listening to Prozac” author Peter Kramer points out: “a reliable finding is that antidepressants work for chronic and recurrent mild depression, the condition called dysthymia. More than half of patients on medicine get better, compared to less than a third taking a placebo.”
“Maybe what antidepressants need, these days, is a defender,” writes Maura Kelly in a 2012 Atlantic article (in which the Kramer quote appears). Kelly points out that while non-pharmaceutical treatments are often recommended for depression, good therapy can be expensive, and following an exercise regimen is difficult for people who have trouble getting out of bed. “In some cases — like mine,” she writes, “years of therapy don’t solve the problem, and neither does daily exercise.”
“The bottom line is that these medications often relieve the patient’s suffering,” Houston psychiatrist John Oldham, then-president of the American Psychiatric Association, wrote in a letter to the New York Times.
Another defender, Dr. Howard Forman, medical director at Montefiore Medical Center in the Bronx, has pointed out that “while psychotherapy is another option to helping people obtain better mental health…cost, availability of experts and time demands” are the main reasons people may turn to antidepressants instead.”
Another reason for rising numbers of people taking these drugs is that 25 to 60 percent of anti-depressants are prescribed for off-label uses, including anxiety, addiction, eating disorders, insomnia, pain, panic disorder, fibromyalgia, OCD and symptoms related to both PMS and menopause. Less common reasons: arthritis, migraine, panic disorder, PSTD and fainting.
The blame on antibiotics for the increasing prescription of antidepressants comes from research on the gut-brain connection: disruption of the healthy balance of bacteria in the gut by antibiotics can produce brain chemicals linked to depression. A Tel Aviv University study looking at health records of more than a million British patients from 1995 to 2013 found one course of antibiotics boosted the risk of depression by about one quarter; while between two and five courses raised the risk by nearly half, according to the Daily Mail.
Besides antibiotics, a host of other drugs with depression as a side-effect include barbiturates and benzodiazepines (for anxiety, insomnia, etc.), beta-blockers and calcium-channel blockers (for high blood pressure and heart problems), opioids (for pain), statins (for high cholesterol) and acyclovir (for shingles and herpes).
The analytic rumination theory comes from research published in PLOS ONE, the peer-reviewed, open-access journal, based on a 20-question test given to almost 600 subjects at McMaster University. “We are seeing more evidence that depression can be a necessary and beneficial adaptation to dealing with major, complex issues that defy easy understanding,” McMaster professor Paul Andrews told Science Daily.
The study concluded that depression may arise when the mind concentrates involuntarily on a complex issue to the point where it allocates resources to analyzing the problem at hand, leading to disruptions in eating, sleeping and social interaction associated with depression. With this understanding, said researcher Skye Barbic, “instead of discussing the disease as a ‘bad thing,’ clinicians maybe be able to help patients have insight about the potential adaptive purposes of their thinking.”
As always, it’s a question of finding the balance. For many people, antidepressants can make a difference.
— Mary Carpenter Mary Carpenter is MyLittleBird’s well-being editor. See more of Mary’s posts here.
TUBERCULOSIS CASES in the United States, while rare, rose in 2015 for the first time in almost a quarter century — thwarting hope of eradicating one of the world’s deadliest diseases from this country. Numbers rose in 29 states and D.C., with D.C. totals remaining in the lowest category (under 36 cases), while more highly populated Maryland and Virginia fall into the next highest: 90 to 600 cases.
“We are really at risk of a resurgence of TB … like we saw in the late 1980s and early 1990s, and potentially worse,” Robert Belknap, president of the National Tuberculosis Controllers Association told the Wall Street Journal. Before that, the numbers of cases had been declining for several decades.
TB is an “airborne” disease that spreads when someone with active TB — versus latent TB, which is detectable by tests but causes no symptoms — coughs, sneezes, speaks or sings; but not from sharing toothbrushes, food or drink, or from kissing. The risk of acquiring TB is related to the duration of exposure — usually longer than three months — and frequency; also to ventilation and degree of intimacy with the affected person.
Within a family, the spouse of the affected person is more likely than the children to catch it. When a school bus driver in rural New York with active TB drove 258 students over several months, 83 children acquired TB with 51 getting the active disease. In countries where TB is endemic, the risk of catching the disease increases only for “long-term travelers,” those remaining for more than three months.
In two cases of infected airplane passengers, the most famous occurred in 2007 when Atlanta lawyer Andrew Speaker took an overseas (long duration) flight without telling anyone he had active, drug-resistant TB — and was later sued by eight fellow passengers in a Canadian court.
Multi-drug resistant TB (MDR-TB), which is increasing around the world, is most often caused when people stop before finishing a full course of antibiotics, and the surviving bacteria that has become resistant to the drug keep multiplying. MDR-TB is the most dangerous form of TB, because it can require difficult, lengthy, expensive and not always successful treatment.
After the Speaker incident, in 2007, the CDC created a “Do Not Board” list (different from the TSA’s “No Fly” list), updated every two weeks, although in 2013 someone on this list managed to board a two-hour flight from Austin, Texas, to Phoenix — with the CDC notifying the TSA only after the plane took off. The passenger was removed in Phoenix before continuing on to Los Angeles. In both airplane incidents, the risk of contracting TB was considered so low that health officials recommended passengers not seek medical care, and no passenger contracted TB.
“To date no case of active TB has been identified as a result of exposure on a commercial aircraft,” according to the World Health Organization — though, “with TB increasing worldwide, there is a small but real risk of infection being transmitted during air flights.” Infectious TB patients are not supposed to travel by air until they have completed at least two weeks of adequate treatment, and patients with resistant TB must be proven by laboratory tests to be non-infectious.
The WHO reported 1.5 million TB deaths world-wide in 2014, more than those killed by HIV/AIDS, as well as 9 million new TB cases. In 2015, the U.S. had 9,563 cases. Compared with the 2014 numbers, Texas had 1334 cases or 5% more; and South Carolina had 104 cases, a 32% increase. Four states — Texas, California, Florida and New York — have one-third of the U.S. population but almost half of reported TB cases.
Of foreign-born TB patients in the U.S., half come from China, India, Mexico, the Philippines and Vietnam. TB screening is required for those seeking permanent residence here but not for foreign-born temporary workers.
A bacterial disease that primarily attacks the lungs, TB can cause a bad cough lasting three weeks or longer, chest pain and coughing up blood or sputum (mucus). It can also infect the kidneys, spine and brain. Because TB was on the wane for decades starting in the early 1970s, U.S. doctors sometimes mistake symptoms, such as bad coughing, for the flu or other conditions.
For most people who breathe in TB bacteria, the body’s immune system prevents the bacteria from multiplying, although these individuals may get sick years later if their immune systems become depressed. The risk of developing active disease following infection is about 5 to 10% during a lifetime. About 85% of people in the U.S. who develop active TB previously had latent infections.
As a result, stopping the spread of TB requires finding and treating the up to 13 million people in this country with the latent disease. Outbreaks in the U.S. occur mostly in homeless shelters and prisons.
Because the drug regimen for treating TB can last up to nine months, many are reluctant to be tested. After an outbreak in a rural Alabama town had gone on for more than two years, a CDC grant enabled local officials to offer residents money — $20 each for taking the TB test, for the visit to learn the results, for getting a chest X-ray, and then $100 for completing treatment. Of 2,257 tested, four had active TB, and there were 170 latent cases.
In Africa, where about 1,500 people die of TB every day, a new method of detecting TB in sputum uses specially trained TB-sniffing rats — also trained to detect landmines. While a human technician can examine 100 samples a day, a “HeroRAT” can examine that number in 20 minutes. In use since the early 2000s, the rats have increased TB detection rates by 45%. With one untreated active-TB patient thought to infect an average of a dozen people/year, the rats have dramatically reduced new cases of TB.
The long-standing goal for the U.S. is to reduce TB to one case or fewer/million people. Meanwhile, when traveling by plane, you could don a mask if you notice coughing and sneezing two rows ahead or behind you — the generally considered area of risk. Or, a more discreet method, coat your nostrils with an antibiotic ointment (like Neosporin) before flying.
— Mary Carpenter Mary Carpenter is the well-being editor of MyLittleBird. See more of her posts here.
EVER FEEL like Gumby? Do double-jointed tricks with your thumbs, remember dropping into splits easily in your youth? Have such difficulty standing for long periods that an hour at a museum is more tiring than one spent climbing the Billy Goat Trail? Also, tired and achy? Have cold hands and feet?
You might have hypermobile joints, which are too loose, move too easily and/or move too far. “You can’t control your joints the way you need to,” according to Mike Robertson. One indicator of hypermobility is difficulty standing on one leg.
Loose joints create strain on soft connective tissues — muscles, ligaments and tendons that are designed to stabilize joints — in turn, making the connective tissue too lax to stabilize the joints and more vulnerable to tearing and pain. While the most common sign is too much flexibility, hypermobile people can also feel stiffness and tension in the joints.
With reduced awareness of the location of their bodies in space, called proprioception,” hypermobile people frequently bang into things and may have been told they were clumsy or awkward — a klutz,” notes local Certified Advanced Rolfer™ and movement therapist Rebecca Carli Mills.
Suffering chronic joint pain and other symptoms related to hypermobility can lead to a diagnosis of Joint Hypermobility Syndrome (JHS), writes Alan Pocinki, hypermobility expert at George Washington Hospital, in a packet requested by his patients “to help educate others about their condition.” JHS affects three times as many women as men, occurs in as much as 10% of the population, and tends to diminish with age.
“Emerging awareness” is how Carli-Mills describes the current thinking about hypermobility, as descriptions and classifications change with new research. People with lax joints fall along a broad spectrum, from those with hypermobility but only mild or no related symptoms — to those more severely affected, some of whom have variations of a rare connective tissue disorder called Ehlers-Danlos Syndrome.
“Remarkably, this process [of tissue damage related to hypermobility] occurs so gradually than many people with JHS do not even notice…when in fact their necks are a mass of knotted soft tissue,” Pocinki writes.
Identifying joints as loose or hypermobile is crucial when choosing good exercises and activities — and avoiding those that can make problems worse. Resistance exercises, called isometric, keep the joints stable while working the muscles. Imagine pushing against a building “as hard as you can as if trying to move it,” writes Kerrie Reed, on Livestrong.com.
The best exercises involve weight lifting and tension bands — increasing repetitions while maintaining low weight or resistance, according to Pocinki: if you can’t do eight repetitions without straining, the weight is too heavy; and, don’t increase weight or resistance until you can do two sets of 15 reps without straining.
Bicep curls should be done with controlled resistance, that is, not relaxing the arm or releasing the weight at any point; and focusing on whole-body alignment to avoid straining a different part of the body, like the lower back, says Carli-Mills.
What’s very important for hypermobility is strengthening the core to decrease the load on susceptible joints, for example, by doing modified Pilates on the mat or ball. Also recommended are quadruped exercises, the most familiar being “bird-dog” — on all fours, stretch one arm out in front and the opposite leg in back, like a dog pointing toward its prey.
For all exercises, engage the body’s stability prior to the movement. Iyengar Yoga poses can provide good stretching, because muscles are engaged in isometric contractions and kept in controlled alignment — what some call “hugging in.”
The worst exercises for hypermobile joints are free-flow stretching like ballet or gymnastics. Anything that involves grabbing a joint and pulling or pushing to “loosen it up,” Pocinki writes. While hypermobile people often feel the need to stretch, in some cases their joints are already stretched as far as they will go — like a rubber band with no more elasticity. Once overstretched, a ligament can’t be corrected, “but you can turn on [activate] muscles surrounding the joint,” explains Robertson.
Among activities, the best for hypermobility are low-impact and improve muscle endurance: swimming, cycling, cross-country skiing, walking and Pilates. The worst: high-impact exercises that involve running, jumping or physical contact, according to Pocinki.
Fatigue and pain are the most common symptoms that accompany hypermobility — caused by poor posture, ineffective movements and “improper muscle recruitment” when performing simple tasks, according to a hypermobility blog. Some hypermobile people use physical or occupational therapy to learn correct movements.
Almost every JHS patient has chronic neck strain because the neck ligaments are too loose to support the neck, which forces the neck muscles to work harder, Pocinki explains. Also the shoulders are so loose and weak that activities using the arm pull on the neck. Other affected joints can cause knee, hip and back pain, tennis elbow, ankle sprains and bunions.
Other JHS-related symptoms: lightheadedness on standing quickly, low blood pressure, headaches, digestive issues, anxiety, nearsightedness or drooping eyelids, unexplained bruises and abnormal scarring, and constant thirst. Pocinki emphasizes that “Many people with loose joints will have no related medical problems at all.”
To assess the degree of hypermobility, the Beighton score uses these movements: bending your little finger backwards; bending your thumb forward to touch your forearm; hyperextending your elbows and/or knees; putting your palms flat on the floor without bending your knees. To diagnose JHS, that score is combined with other criteria, many related to pain such as the number of joints affected, the duration of pain, back pain and soft-tissue problems such as tendonitis.
While increasing muscle tone and stability can be a slow process, “people improve more quickly if they give up things that are bad for them, like running and stretchy hot yoga, while following a consistent program in good isometric exercise,” says Carli-Mills. And whenever possible, she suggests: engage the glutes and abs.
Another suggestion: when standing in line, spread weight evenly over the feet — think “leaving big foot prints” — then increase pressure through the feet into the ground — creating deeper and bigger foot prints; then allow this pressure to spread upwards through legs and hips, without locking the knees, through the top of the head. As she puts it, “Reach towards sky, connect the sky to the ground.”
Do something every day, even when tired, says Pocinki: a minimum of five minutes of light weights for shoulder strengthening and five minutes of isometrics for core strengthening. With another five minutes, add the bird-dog.
From the British Hypermobility Syndrome Association, the advice is Fidget! And avoid staying in any one position for more than half an hour.
Be aware of surfaces, says Carli-Mills. In movie chairs that slant backwards, for example, stuff your jacket into the back. And “soft lumpy sofas are bad news” because a JHS person’s alignment slides easily out of place.”
Finally, she advises, “Bring more mindfulness to movement and action to activate the nervous system in a different way.”
— Mary Carpenter Mary Carpenter is the well-being editor of MyLittleBird. See more of her posts here.
AFTER YEARS of counting myself among the “worried well”— those who believe their memory is slipping despite high scores on cognitive tests — I enrolled in a clinical trial. The potential upside: a PET (Positron Emission Tomography) scan at no charge, versus the out of-pocket cost of about $3,000.
PET scans can detect amyloid plaque, one of two signature physical changes in the brain linked to Alzheimer’s Disease (AD) that until recently have been observable only after death. Amyloid plaque is suspected of damaging and killing brain cells long before clinical signs of dementia associated with AD appear.
My goal in signing up for the “A4” (Anti-Amyloid Treatment in Asymptomatic Alzheimer’s Disease) study: to have experts monitoring and measuring over several years so I could relax.
Among potential downsides of the trial, however, the worst was that the PET scan could document early signs of AD, thereby moving me to the “worried less-well” category. Another negative: a probably painful spinal tap to examine cerebrospinal fluid (CSF) — optional, but I’d said yes in the interest of acquiring the full battery.
Also distasteful but mandatory: monthly injections of either saline solution (for the control group) or a drug that risked unpleasant side effects and had already failed several trials of efficacy. Because several such drugs targeting amyloid plaque have failed to alter the course of AD in large trials, some experts worry that amyloid appearing on a PET scan has been accumulating for decades, meaning it’s too late for effective treatment and thus for the usefulness of these scans.
A final drawback to the A4: required trips to Georgetown Hospital — good coffee, horrendous parking —starting with four “screening” visits. The first one lasted four hours and, worse, required the presence of an incredibly good-hearted friend, who would provide feedback on my cognitive function for the study’s duration. Post-screening would include more than ten visits, lasting four to five hours each over several years, hopefully without imposing each time on my friend.
Screening visit #2 was the PET scan. Different from CAT scans and MRIs that provide “structural imaging” to determine the size and shape of organs and bones, PET scans provide “functional” images to measure such bodily functions as blood flow, oxygen use and sugar metabolism. PET scans are also categorized as “molecular imaging” because they employ a radioactive tracer. For AD evaluations, the tracer binds to beta-amyloid in the brain, creating “bright” or “hot” spots where large amounts of tracer accumulate.
For my PET, I lay in a darkened room on a narrow platform and am told not to budge. As the radiotracer was injected into my arm, the scanner moved over me and I fell asleep for about half an hour. Not until visit #3 a few weeks later did I learn the results: my PET scan was “clear” of plaques. I was kicked out of the study, ecstatic — at least for now.
AD has traditionally been diagnosed based on cognitive tests like the MMSE (Mini-Mental Status Examination) — the ones I still ace, more or less. But doing poorly on these can indicate that severe damage to the brain has already occurred.
Medical centers such as the University of California at San Francisco (UCSF) have “offered Alzheimer’s disease assessment with amyloid PET scanning for patients with memory complaints” since 2003. According to the UCSF website, “Amyloid PET imaging represents a potential major advance in the assessment of those with cognitive impairment.”
PET scan evidence of early amyloid plaque formation or changes in beta-amyloid levels is most useful to confirm or disprove the AD diagnosis for patients with mild cognitive impairment — rather than for those who have been clearly diagnosed. Questions about the scans persist, however, because many people whose autopsies showed amyloid plaques had exhibited no symptoms of cognitive decline. Clinical studies are now underway to assess the value of PET scans in diagnosing early AD — and confirmation would encourage insurers to cover the scans.
Besides amyloid plaque, the other signature sign of AD is “neurofibrillary tangles” composed of tau proteins that have been tangled and twisted, which impairs their ability to support synaptic connections. Although higher levels of tau protein are present in almost every aging brain, it’s the spreading of tau, for example, into the neocortex, that is associated with serious declines in global cognitive function.
Spreading tau has also been linked to the presence of amyloid plaques in the brain. Many experts believe that “the accumulation of amyloid serves as the kindling for other events” that set off early AD, as Dr. Eric Reiman of the Phoenix-based Banner Alzheimer’s Institute told the New York Times.
“Amyloid may somehow facilitate the spread of tau, or tau may initiate the deposition of amyloid,” explains Berkeley researcher William Jagust. “We don’t know…when amyloid starts to show up, we start to see tau in other parts of the brain [which] may be the beginning of symptomatic Alzheimer’s disease.”
Another area of concern: “brain cells affected by dementia consume less energy than normal brain cells” — which over time can decrease overall brain volume or change the density in affected parts of the brain — according to the Society for Nuclear Medicine and Molecular Imaging (SNMMI) website. “Molecular imaging excels at detecting the cellular changes…often well before structural changes can be seen on CT and MR images.”
Some believe that diagnosis of early Alzheimer’s improves considerably when changes detected by PET scans are combined with elevations in beta-amyloid and tau proteins detected in the cerebrospinal fluid. The hope is that molecular imaging may eventually help monitor disease progression and assess potential treatments.
Meanwhile, “Dramatic Decline in Dementia” was a recent banner headline on the respected medical website STAT, announcing a study of more than 10,500 adults age 65 or older that showed the percentage with dementia, including Alzheimer’s Disease, declined from 11.6% in 2000 to 8.8 percent in 2012.
Increased education among the 2012 group may be the most important explanation, according to University of Michigan researchers. Education “can produce greater cognitive reserve, in which people have enough backup synapses and neurons that losing some to Alzheimer’s still leaves them short of dementia,” Sharon Begley explains in the STAT article. The longitudinal Framingham study also recently produced evidence of the falling risk of dementia among older adults — by about 20% every decade between 1977 and 20008.
If, as currently believed, studying foreign languages and playing musical instruments are the best ways to forestall dementia, there’s a lot more to be done than worrying or spending a sleepy half-hour in a PET scan machine.
— Mary Carpenter Well-Being editor Mary Carpenter recently posted on the success of non-AA rehab. See more well-being stories.
ANTIGUA, MALIBU, Tucson, anyone? The attraction of a four-week stay at an upscale resort with the likelihood of a celebrity or two is undeniable — even if the days are packed with therapy based on the 12 steps of Alcoholics Anonymous (AA), the monthly price tag as high as $50,000, and the likelihood of success very low.
Long-term success rates of AA-based-treatment — including resort rehab and regular 12-step meetings — may be as low as 5%, according to retired Harvard psychiatrist Lance Dodes in his book, “The Sober Truth: Debunking the Bad Science Behind 12-Step Programs and the Rehab Industry.” Furthermore, low-cost publicly funded clinics often have better-qualified therapists and better outcomes than high-end residential centers, according to Anne Fletcher in her book, “Inside Rehab.”
A 2012 report from Columbia University’s National Center on Addiction and Substance Abuse “compared the current state of addiction treatment to general medicine in the early 1900s, when quacks worked alongside graduates of leading medical schools,” according to a 2015 Atlantic Monthly article by Gabrielle Glaser. The report’s conclusion: “the vast majority of people in need of addiction treatment do not receive anything that approximates evidence-based care.” Glaser also cites “The Handbook of Alcoholism Treatment Approaches,” published more than ten years ago, that ranks AA 38th out of 48 methods.
Of more than 13,000 rehab facilities in the U.S., however, as many as 80% follow the Alcoholics Anonymous model and recommend AA follow-up — 90 meetings in 90 days is the mantra — for what’s now called “Alcohol-Use Disorder” (AUD). Many people have been helped by AA and by the ready solace of its ongoing groups.
About 18 million adults in the U.S.— as many as 20% of patients seen in primary care of hospital settings — abuse alcohol, and the numbers are rising, according to the National Institute for Alcohol Abuse and Alcoholism (NIAAA). One definition of AUD: having developed a high tolerance for alcohol and experiencing withdrawal symptoms if its use is suddenly stopped.
Research-based conclusions about AUD that run counter to the AA model are ignored by most practitioners, says addiction psychiatrist Mark Willenbring, director of treatment research at NIAAA from 2004 to 2009 and founder of the Minnesota outpatient clinic Alltyr. “When the facts change — and they’ve changed a lot — the minds have not,” he told the New York Times.
AA keeps no records of participants but claims to have more than two million members worldwide. According to the “Big Book,” AA’s bible, the program works for 75% of those who go to meetings. Critics deem this claim a tautology since most of those who go to meetings have already stopped drinking and attend to maintain rather than achieve sobriety — but in fact all that’s actually required of attendees is the intention to stop, and willingness to join in the group’s serenity prayer is considered a personal pledge.
AA’s blame-the-victim ethos considers alcohol abuse a personal failure of will. According to the Big Book, “Those who do not recover are people who cannot or will not completely give themselves to this simple program…who are constitutionally incapable of being honest with themselves.”
This morality stigmatizes people who fail to overcome addiction — as it does with obesity. Fear of the stigma as well as the abstinence-only goal of AA keep people from asking for help until their problems become so serious that treatment is more challenging. Only about 10% with alcohol and substance-use disorders ever seek treatment.
More successful approaches than AA, available since the early 2000s, are individualized; involve medical professionals — who can treat co-occurring disorders such as depression as well as prescribe anti-abuse medication; and offer help for as long as necessary — usually a lot longer than 28 days.
A key reason for failure of the 28-day/AA model is dual diagnoses — that is, when addiction is accompanied by disorders of depression, anxiety, or more serious conditions like bipolar disorder and schizophrenia. Co-occurring conditions affect approximately 37% of those with AUD and 53% with drug addictions, according to the National Alliance of Mental Illness.
In fact, treating the co-occurring conditions with medication and/or therapy can reduce cravings for alcohol. Most experts agree that about half of a person’s vulnerability to alcohol-use disorder is hereditary and that co-occurring conditions play a role.
But the AA model approach advises against taking any anti-abuse medication as well as potentially “mood-altering” drugs; many AA participants believe they should refuse all medicine, even aspirin for headaches. Medication-assisted-treatment (MAT) “has never been quite as controversial a subject as it is today,” according to the Substance Abuse and Mental Health Services Administration website. Despite increasing evidence of MAT’s effectiveness, only 1 to 2% of people treated for alcohol-use disorder receive anti-craving medication.
The drug Antabuse, which causes nausea when combined with alcohol, can be given only to patients who have completed withdrawal from alcohol and are committed to abstinence. In contrast, Naltrexone, which blocks the opiate receptors involved in the pleasurable effects of drinking as well as in cravings for alcohol, is considered a “treatment” drug and can be offered to those struggling to recover.
Over time, constant consumption of alcohol changes the brain, in particular altering the release of chemicals such as GABA and dopamine that create the feelings of warmth, contentment and good humor associated with alcohol; and strengthening the synaptic connections that increase the likelihood of thinking about and eventually craving alcohol, until drinking becomes compulsive.
Naltrexone has been shown to reduce drinking and increase abstinence in more than a dozen clinical trials, including one large scale NIAAA-funded trial published ten years ago. Because it’s available in an inexpensive generic form, however, drug companies are not promoting it. Still, AUD experts are baffled by its limited use.
For her article, Glaser tried Naltrexone (ordered with no RX online) and, sipping her evening glass of wine, “felt almost nothing — no calming effect, none of the warm contentment that usually signals the end of my workday … I had never found wine so uninteresting.” After taking the drug for several more nights, she wrote, “I no longer looked forward to a glass of wine with dinner.” She also lost several pounds, noting that an opioid antagonist is being tested on binge eaters in Europe.
Resort rehab also runs up against research indicating that most individuals need at least three months of treatment to significantly reduce or stop their addictions. Those with co-occurring or long-standing addictions can require 12 months or longer. Which is why successful rehab programs are local and available as long as and whenever needed.
At Alltyr, Willenbring’s Minnesota clinic, addiction is considered a chronic medical condition, and treatments include antidepressants, anti-relapse medications and psychotherapy — for as long as needed. “You don’t treat a chronic illness for four weeks and then send the patient to a support group,” Willenbring said. These individuals need treatment “that is individualized and offered continuously or intermittently for as long as they need it.”
Among patients who were helped at Alltyr, one woman had been in and out of rehab 42 times, and one young man had tried more than 20 abstinence-based programs, attempted suicide and overdosed on heroin.
AA’s one-size fits all approach “was originally intended for chronic, severe drinkers — those who may, indeed, be powerless over alcohol,” notes Glaser. But only about 15% of those with alcohol-use disorder are at the severe end of the spectrum. And whereas AA considers alcoholism a progressive disease that can only get worse, in fact as many as 20% may go on to drink at low risk of becoming more dependent, she wrote.
Any changes in this picture make news, such as when the Hazelden Betty Ford Foundation, previously an AA-only model, announced it would offer Naltrexone. But that was in 2006 — and there has been little movement since.
— Mary Carpenter Mary Carpenter, MyLittleBird’s well-being editor, last wrote about the dangers of hepatitis C.
FOR BASKING in the love — but mostly in the drugs — of the late 1960s and early 1970s, baby boomers are paying the price with hepatitis C — what some are calling an epidemic-in-the-making. Infection rates for white Americans in the boomer age group with the often symptomless hepatitis C virus (HCV) might be as high as 3%, double the national rate.
NIH hepatitis C researcher Leonard Seeff calls it “an iceberg problem.” Compared to those patients currently experiencing symptoms of HCV, probably ten times that number are walking around with no idea they’re infected. In his St. Louis practice, hepatologist Bruce Bacon sees 8 to 10 new HCV patients a week, among whom up to 30% claim to have never experienced any of the risk factors.
In 2012 the CDC began “recommending” that everyone born between 1945 and 1965 be tested. Since then, states including New York, Massachusetts, Connecticut, Colorado, and most recently Pennsylvania have passed laws requiring that boomers be offered hep C testing when receiving healthcare services. Since the CDC’s recommendations were issued, DC region private medical practices — which added hepatitis C testing as part of the annual physical exam — have uncovered handfuls of unsuspected cases.
While HCV can cause an acute infection, the chronic disease that occurs in 75 to 80% of cases can last decades before symptoms occur and liver damage begins. As many as 20% of those infected develop cirrhosis, and 1 to 5% will die of liver disease or liver cancer — making HCV a leading cause of liver cancer and the leading cause of liver transplants. Once diagnosed, in hindsight some people remember unusual episodes of fever, fatigue, loss of appetite, nausea, dark urine and joint pain, which can range from mild to severe.
The most common route of hep C transmission is shared needles for IV drugs like heroine — which has caused an infection rate among African American baby boomers as high as 6%. But because testing for the virus in the nation’s blood supply didn’t begin until 1992— the disease itself wasn’t identified until 1989 — routes of transmission have included everything from contaminated blood transfusions, medical equipment and procedures to unsterilized tools for tattoos and acupuncture and even sharing a cocaine straw, toothbrush or razor blade.
According to the CDC, however, the reason that people born from 1945 to 1965 have high rates of hepatitis C is not completely understood. Also not well understood is how approximately 15% to 25% of people who get the virus are able to clear it from their bodies without treatment and never develop chronic infection. As yet, no HCV vaccine exists.
Each year, more than 10,000 Americans die of hep C, a figure that is predicted to triple over the next two decades. About four million Americans are currently infected with the disease, compared to around one million with HIV. Because HCV can take several decades to cause liver disease, the CDC anticipates a spike in people with hep C needing medical care over the next 20 years.
The timing of the CDC’s recommendations coincided with the first drugs coming down the pipeline that can definitively “clear” the virus from the blood. In 2016, a new drug called Epclusa has shown success with the rarest and most difficult to treat hep C strain — or genotype — while new combination drugs target all six genotypes.
High price tags on these drugs, more than $70,000 for a 12-week treatment to completely clear the virus, suggest that the drug companies may have spurred the CDC to issue its recommendations. On the other hand, most people pay a reduced price because of private deals between drug companies and insurers.
More importantly, eliminating this virus could reduce the enormous financial burden of HCV on the U.S. health care system, especially as numbers soar of hepatitis C sufferers whose livers have been destroyed by cirrhosis and who find donors for transplants.
The eradication of smallpox is estimated to save 5 million lives annually; and vaccinating 80% of the world’s children against polio has reduced annual numbers of cases by almost 80%. The savings to the U.S. from identifying and treating those with HCV — especially considering the numbers of sufferers with livers destroyed by cirrhosis who require transplants — can only be imagined.
— Mary Carpenter Mary is the well-being editor of MyLittleBird. She most recently wrote about how D.C. suffers from seasonal allergies.
FIRST COME sniffles and sneezes. Then, an oft-heard refrain: “I NEVER had allergies until I moved to DC!”
The likelihood of developing seasonal allergies (as distinguished from those to food, dust or other things) in the DC area is due to the sheer numbers of triggers here—with tree pollen starting off the spring season, grass pollen in the summer and weed pollen in early fall followed by leaf mold. U.S. Army microbiologist Susan Kosisky told the Washington Post, “We’ve got something for everybody here. . . . If you come to the Washington, DC, region without an allergy, there is a chance you will leave with one.”
In the allergy ranking of U.S. cities, numbers of allergenic grasses, trees and weeds are key variables, as are seasonal and other changes from year to year. According to Greer allergy maps, DC is near the top—with 14 grasses, 35 trees and 14 weeds, for a total of 62 seasonal triggers—falling between other notably allergenic cities of Houston at 58 and Knoxville at 64.
Being constructed on a swamp gives DC a comparably longer growing season with less likelihood of a killing frost to interrupt the season once it starts. Also, DC’s trees include many oaks, notorious for producing pollen that hangs around for a long time rather than dispersing quickly.
While each allergen has a yearly “crop,” some years it’s a bumper while others it’s mild,” explains Nutley, New Jersey, allergist Alan Goodman. Spotting the first green willows of springtime tells him when the office phone will start ringing. After 25 years in this specialty, he says: “I know it’s a bad season when the ringing phone never stops.”
Physical proximity to specific allergens is the only way to trigger seasonal allergies, which can develop following the first exposure over a two- to seven-year period. For one man who’d never had any allergies, it took three years after moving from Hong Kong to DC for seasonal allergies to become so severe that swollen tissues in his nose caused tiny blood vessels to break easily, resulting in frequent nosebleeds.
For some people, seasonal allergies that seem to arise anew in adulthood can be traced back to earlier sensitivities. I once put myself among new-to-DC allergy sufferers and then remembered having such bad poison ivy as a child that I wore gloves at night to keep from scratching.
Symptoms of allergic rhinitis—runny nose, sneezing, scratchy throat and itchy eyes—caused by seasonal triggers can be distinguished from those of colds and flu primarily by patterns of occurrence: arising during specific seasons, worsening after time spent outdoors and improving after nights with the windows shut. Symptoms particular to allergies include itchy eyes, absence of fever and clarity of the mucus.
Colds, by contrast, usually worsen over time and then improve; produce yellowish mucus; and can be accompanied by fever. And fever above 102 can indicate flu. Difficulty swallowing suggests strep throat, which requires a test because treatment includes antibiotics. Fatigue is common to all of these. But diagnosis can be tricky if something else occurs at the same time as an allergic reaction.
Allergy symptoms appear to be increasing around the world. Some blame higher concentrations of airborne pollutants. Others subscribe to the “hygiene hypothesis,” that life in developed countries became so sanitized that people’s immune systems didn’t develop correctly. The theory is controversial because greater use of antibiotics and indoor plumbing occurred in the same period. The good news: Immune responses weaken with age, making seasonal allergies less likely to arise in a person’s 30s and 40s, and especially after age 50.
Another villain is increasingly long pollen seasons caused by effects of global warming, such as rising temperatures and greenhouse gases. Research on the length of ragweed pollen seasons from 1995 to 2009 found that, compared with almost no increase in the three southernmost cities (in Arkansas, Oklahoma and Texas), seasons lengthened in Nebraska, Wisconsin and Minnesota cities by 11, 12 and 16 days, respectively, with a 27-day gain in the northernmost city in Canada. Though not included in this study, DC is closest in latitude to Nebraska.
Shorter springs—when spring arrives late—compress the allergy season, so that trees are pollinated later but more quickly, and grass pollen comes toward the end of that with no break. In what some call a “pollen tsunami,” peak DMV pollen concentrations can reach 4,000 particles per cubic meter of air.
For an individual to develop new seasonal allergic responses, the immune system must first identify as harmful such allergens as pollen and mold. In response, inflammatory chemicals such as histamine are released, causing symptoms that involve the nose, eyes, skin and digestive system.
Genetics affect an individual’s chances of developing allergies: Responses to the same allergens occur in 70% of identical twins and 40% of fraternal twins. Allergic parents are more likely to have allergic children, and those children are likely to have more severe allergies. What experts don’t entirely understand, however, is why someone develops an allergic reaction to certain allergens but not to others.
To combat allergy symptoms, the best non-sedating antihistamines for many sufferers are Claritin and Allegra, according to allergist Goodman, who advises patients to go for the cheapest available—as low as $12 per year at Costco. While some combination drugs include “decongestants,” those do not target the allergic reaction–which antihistamines do–and can cause side effects including blood-pressure problems and insomnia.
Even with medication, some patients spend weeks in the hospital, including days in the ICU. For the worst cases, “immunotherapy” using injections of specific allergens can alleviate or end symptoms. Extremely time-consuming—with regular shots starting at once a week and lasting over several years—and expensive, however, immunotherapy is usually worthwhile only for the most seriously afflicted.
Good weapons for most seasonal sufferers involve limiting exposure. If grass is the problem, don’t mow or, if you must, use a mask. After being outdoors, take a shower and throw clothes in the wash. Keep the windows closed. Best of all, if possible: Get out of town for the worst periods, and don’t come home until they’re over.
— Mary Carpenter
Mary Carpenter is the well-being editor of MyLittleBird. Her most recent post was on new treatments for migraine sufferers.
DESPITE EXCITEMENT over the years about one new migraine treatment after another, most sufferers have found little relief. In the early 2000s came the discovery that laboratory-produced antibodies might prevent these excruciatingly painful experiences.
Since then so-called migraineurs have waited — patiently and painfully — as the new drugs made their way through FDA testing process, only recently arriving at Stage III trials, which are large human studies of safety and efficacy. Now people are talking about widespread availability “later next year.”
Migraine headaches affect 10-12% of females and 6-8% of males, and are among the world’s most prevalent neurological conditions. Migraines can be inherited, and some people are “superresponders,” such as someone who had a migraine every day from early childhood into her mid-20s.
The migraineur’s brain is like a car with a heightened alarm system that “goes off simply because you walked close to it,” says Mayo Clinic neurologist David Dodick. Often more than headaches, migraine attacks are complex events that cause brain activity to be “completely dysregulated,” Dutch neurologist Michel Ferrari told Science magazine.
Since the early 20th century, dilated veins and arteries in the brain have been blamed for migraines — in part because patients report throbbing blood vessels in their head during an attack. Drugs introduced in the 1990s called triptans selectively constrict blood vessels in the brain and remain the most widely prescribed treatment. While they can lessen the severity of headaches, they don’t reduce the overall number and, when taken frequently, can cause even worse headaches. Other treatments include regular injections of botulinum toxin type A, and drugs such as beta-blockers, anticonvulsants and calcium-channel blockers.
Then came fMRIs (functional magnetic resonance imaging), which showed no relationship between abnormal blood flow in the brain and the pain of migraine attacks. What did occur was the release of a molecule called CGRP (calcitonin gene-related peptide), found in brain pathways that process pain and in brain regions that regulate blood flow.
“This is the most exciting thing we’ve seen so far,” said Swedish neurologist Lars Edvinsson, who studied blood taken from the jugular veins of people coming to the Emergency Room for severe migraines. Besides expanding blood vessels, CGRP turned out to be a previously unknown pain-signaling neurotransmitter.
Rather than patterns of abnormal blood flow, it was rising levels of CGRP that triggered an attack. In one study, CGRP injected into the blood of migraineurs produced migraine-like headaches whereas non-migraineurs had little reaction.
The first approach to treatment used compounds that block CGRP’s receptors, but these trials were stopped due to side effects. The next step was antibodies, because they can be very specifically directed at substances causing problems. Monoclonal antibodies created in the lab attacked CGRP and also mobilized the body’s own immune response.
Because these antibodies are too large to penetrate the blood-brain barrier and thus circulate only in the peripheral nervous system — their successful treatment of migraines led to the exciting discovery that neurological conditions could be treated from outside the brain, creating hope that other pain disorders like cluster headaches and fibromyalgia might also be treated this way.
“It is the only hope on the horizon, Cornell neurologist Joseph Safdieh told the New York Times. For a subset of superresponders, just one injection of CGRP-blocking antibody stopped migraines entirely for six months.
Phase I and II trials on several thousand people over six-month periods have shown no significant side effects. Said corporate neuroscientist Corey Goodman: “I don’t think it’s too early to start talking about a cure for some patients suffering from this debilitating disease.”
Others are skeptical. “If CGRP really is a fundamental mechanism, you would expect a much higher proportion of patients to be completely free of attacks,” says Ferrari. Others point out that trials lasting longer than six months are needed to insure the safety of long-term use: because CGRP dilates arteries throughout the body to maintain blood supply to the heart and brain, blocking CGRP could amplify the effects of a minor stroke or cardiac incident. Or it could cause high blood pressure that affects the kidneys or lungs.
Also, because other factors such as stress play a role in spurring migraines, some suspect these complex events could be symptoms of several different conditions. Although one-quarter of migraine sufferers are male, female hormone fluctuations appear to play a role. Tennis player Serena Williams has blamed some losses on “menstrual migraines.” And a medical editor who had terrible migraines before almost every deadline said hers ended entirely with menopause.
What gives sufferers the best hope is that four companies are currently competing to get the first monoclonal antibody drug onto the market.
— Mary Carpenter Mary Carpenter is the well-being editor of MyLittleBird. Her most recent post was on the high costs of health care for women.
SOURCES: (1.) PsychCentral, (2.) Glaucoma Research Foundation, (3.) Hartford Medical Group, (4.) Prevention, 9 Things You Need To Know About Getting Your Tubes Tied, Jan 25, 2016 (5.) Breastcancer.org (6.) Wall Street Journal, Young People Also Weigh Surgery to Relieve Ugly, Painful Bunions, Jan 21, 2013 (7.) University of Colorado Hospital Graphic courtesy vitals.com
COSTS FOR HEALTH and personal care have long been higher for women compared to men — in fact, higher than many may suspect. (more…)