EVERY SUMMER G.M. drives about eight hours north from DC and takes a ferry to the island where she spent childhood summers, and where her grown children are willing to travel many miles to join her. But for the past few years, during the first week or longer on the island, something happens to G.M.’s mouth.
—
Her tongue swells and little sores develop on her tongue and the inside of her lips, making it hard to talk with extended family members—and difficult to eat. Mealtimes are challenging. Especially unpleasant is dry, spicy or salty food, as are the first few minutes in salty ocean water that stings her mouth.
—
For a swollen tongue, the most obvious culprit is an allergic reaction. Histamines flood the bloodstream—called angioedema—swell the tongue and, in severe cases, close the throat, causing life-threatening anaphylaxis.
—
Although G.M.’s diet on the island appears exactly the same as in DC, she always eats plenty of food on the “hypersensitivity reaction” list—in her case: nuts (walnuts and almonds), fruits and vegetables (avocados and tomatoes), milk, eggs, fish (salmon) and shellfish (lobster). Flavorings such as cinnamon, peppermint and menthol in toothpaste as well as candy can also trigger reactions.
—
Discounting allergies, the causes of most other mouth issues either involve swollen tongue but no sores; or sores on the tongue —but not the lip—which make the tongue uncomfortable though not usually swollen. For most conditions, the list of causes includes stress.
—
At a routine checkup after her mouth recovered, G.M’s dentist was pretty set on the diagnosis of “geographic tongue,” in which the papillae or taste buds become inflamed and then disappear, causing the tongue to look red and shiny. Splotchy bare patches on the tongue, which can look like continents on a map, can come and go, change quickly and last up to a year. Pain with geographic tongue comes from sensitivity to hot, spicy or acidic foods and to some toothpastes.
—
Another diagnosis candidate is “lie bumps,” or transient lingual papillitis —mythically linked to telling lies—which are painful and “extremely common” but not well understood. Also, lichen planus is a rare rash that can itch and looks like raised red bumps or lacy, white patches. Possible causes of both include diet that is highly acidic (lots of fruits and vegetables), sugary and/or spicy; and trauma like biting the tongue.
—
By themselves, mouth sores (which can also cause pain in the tongue but not swelling) are most often cold sores from Herpes simplex infection; or canker sores, white or yellow sores linked to food ingredients (especially in spicy food); to vitamin deficiencies, notably vitamin B-12; and to infections.
—
Treatment for all mouth problems starts with what to avoid: spicy and salty food; mouthwash that contains alcohol; and toothpaste with additives, notably sodium lauryl sulphate, but also whitening agents and heavy flavoring. The best is toothpaste for sensitive teeth—and a soft toothbrush.
—
Anesthetic, numbing gels can relieve mouth discomfort, as can a rinse made with salt or baking soda. For bumps, topical treatments can protect them with a bandage-like covering, and a paste made with baking soda or milk of magnesia can help with pain.
—
G.M. didn’t believe she’d found the best diagnosis, however, until her research led to “dry mouth.” Besides having a very dry mouth, symptoms include inflammation of the tongue, called glossitis; painful tongue, glossodynia; and taste disorders, dysgeusia—all of which affected G.M.
—
What impressed her was the inclusion of her most unpleasant and inconvenient issues: difficulty speaking as well as “swallowing and chewing —especially dry and crumbly foods such as crackers”—crackers were the worst for her. Also important was the increased need to drink water, especially at night.
—
When salivary glands aren’t working well enough to keep the mouth moist, xerostomia is most often linked to side effects of medications, including the Wellbutrin G.M. takes. For most who take the offending medications, dry mouth is a small price to pay.
—
Dry mouth is also a symptom for systemic conditions such as hypothyroidism and Parkinson’s disease as well as autoimmune diseases, such as Sjogren’s syndrome, diabetes, lupus and rheumatoid arthritis.
—
But in G.M.’s case, the biggest offender may be what she does on any long car ride. She drinks as little as possible to avoid needing extra bathroom breaks. To stave off sleepiness, she skips meals, instead eating a variety of chocolates, a granola bar, popcorn, and maybe an apple—while specific advice for dry mouth sufferers includes “decreasing your fermentable carbohydrate intake, especially for sticky foods such as cookies, bread, potato chips, gums, candies.”
—
Another trick to help stay awake—and because late July temperatures on the drive are always over 90 degrees—she turns up the air-conditioner fan, which produces very dry air. And then there’s the stress of packing and driving—as well as the immense relief brought by drinking cool liquids and sucking ice chips, which is a mouth-discomfort remedy advised mostly in cases of dry mouth.
—
Adequate saliva is important not only to aid chewing and swallowing but also to enhance the ability to taste; its enzymes aid in digestion; and it helps prevent tooth decay.
—
For dry mouth in particular, remedies focus on increasing saliva with chewing gum or mints—preferably those containing Xylitol to avoid sugar—as well as using mouthwashes and sprays, especially during the night and whenever drinking excess water is inconvenient. Among favorite recommendations for G.M. are breathing through the nose, also good for reducing stress; and eating carrots.
—
G.M.’s dentist agreed that her collection of symptoms was intriguing —“your teeth look fine, but this is exciting”—and suggested she consult an unfamiliar specialty, oral medicine, when her condition returns.
—
That condition occurs, however, only on an island with no specialists at all, even a dentist. Meanwhile, she has stocked up on dry-mouth products, including Sensodyne True White toothpaste, Oasis spray for nighttime, and Xylitol-containing Spry Gems mints and Biotene lozenges —and she has more to try. She also plans to change her driving routine, or at least to skip the popcorn.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
NIGHT OWLS are finally getting some respect: an official sleep chronotype, which refers to “individual tendencies toward the timing of activity and rest each day;” and some evidence that they “tend to be more productive and have more stamina during the day.”
“Humans can be categorized as early (EC), late (LC) or intermediate (IC) chronotypes,” according to researchers in Aachen, Germany. Beyond sleep/wake timings, chronotypes show distinct patterns of cognitive performance, gene expression, endocrinology and lifestyle.”
The news is not all good for night owls, who tend to weigh more, have higher blood pressure and die sooner than early risers. In the Aachen study, their brain scans showed less white matter, which raises their risk of depression, schizophrenia and impaired cognitive function.
By contrast, larks—especially very “short-sleepers,” who sleep less than six hours a night—tend to be optimistic and driven, and resilient against stress and pain, according to UCSF neurologists Louis Ptacek and Ying-Hui Fu, who studied genetic differences in two families, each with some members who “never slept more than six hours a night.”
“Why some people are up with the lark while others are night owls is because of differences in both the way our brains react to external light signals and the normal function of our internal clock,” explained Exeter geneticist Samuel E. Jones.
Because the body-clock cycle is slightly longer than 24 hours, the retina plays a key role in realigning the body clock slightly each day, the researchers found. It confirmed the higher risk for night owls of mental health problems but did not support strong links to diabetes or obesity.
Understanding the “genetics of sleep and activity timing” in the general population offers insights into possible therapy for those with insomnia and aberrant sleep chronotypes, such as Delayed Sleep Phase Disorder (DSPD), according to Mass General anesthesiologist Jacqueline Lane.
Up to one-third of people living in industrialized countries suffer from insufficient sleep, which interferes with the body’s ability to repair tissue, synthesize hormones and grow muscles. Poor sleep can also cause epigenetic changes in DNA, according to a study on the impact of night shifts on 49 “healthy, full-time doctors.” Genetic analysis of those on call overnight showed more DNA breaks and lower “baseline DNA repair gene expression.”
The most recent age-specific, sleep durations, recommended by the National Sleep Foundation, divided adults over age 25 into two groups and added a “may be appropriate” category. For those 64 and under, the “may be appropriate” range was 6 to 10 hours, with 7 to 9 hours “recommended”; for those 65 and older, “may be appropriate” ranged from 5-6 to 9, with “recommended” between 7 and 8.
With D.S.P.D., a “circadian rhythm disorder,” the entire cycle is delayed. Sufferers have difficulty falling asleep but no trouble obtaining a full night’s sleep if they sleep very late the next day, Montefiore Medical Center sleep specialists Shelby Freedman Harris and Michael Thorpy wrote in a New York Times blog. In contrast, those with insomnia usually have some combination of difficulties falling asleep, staying asleep and waking too early, and of feeling insufficiently rested in the morning.
“Chronotherapy” for DSPD (also called delayed sleep phase syndrome) involves delaying the sleep period by two or three hours for each cycle until bedtime comes around to the one desired—but requires patients to sleep during the daytime for several days.
Alternatives include bright-light therapy in the morning with a light box (10,000 lux) for an hour or two—or sunlight; and taking melatonin early in the evening to “pull the circadian drive earlier.”
While DSPD most often affects young adults, the reverse problems of Advanced Sleep Phase Disorder often occur among older people, who go to bed very early (6 to 9pm) and wake very early (2am to 5am)—and who complain of fatigue in the late afternoons.
Testing for sleep disorders usually begins with a sleep diary. “Actigraphy,” using a wrist motion monitor to record activity for days or even weeks, or spending a night in a sleep clinic can help confirm the problems.
Besides bright light therapy, behavior therapy involves keeping to regular sleep-wake times and avoiding naps, as well as exercising and avoiding caffeine and nicotine within several hours of bedtime.
For night owls, too, well-timed, bright morning light can help shift their habit, although Charlottesville nurse practitioner Ellen Wermter would first ask the question: “Do you really need to make the shift?”
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
PROPRIOCEPTION— the sense of where our bodies are in space—depends on receptors in the joints and elsewhere that record the position of body parts in relation to one another. Proprioception is the ability to know, without looking, if one arm is above the head or hanging by the side of the body.
Information about proprioception also comes from receptors in the skin that respond to stimuli, such as pressure, temperature, vibrations and pain. And visual and auditory input helps pinpoint the body’s position relative to surrounding objects and the horizon, and to environmental sounds.
Proprioceptive feedback is essential for controlled movement. For a man with diminished proprioception following a severe infection, “his limbs moved, but he had no control over them. He felt disembodied, as if he was floating in air.”
Most proprioception assessments involve removing vision—with eyes closed or in a dark room: In the “finger-nose test,” touch your forefinger to your nose; in the “thumb-finding test,” touch the tips of your thumbs together. Or ask another person to move your big toe up or down and tell them which way they have moved it.
Poor proprioception can explain the clumsiness of kids during a growth spurt who haven’t yet adjusted to their new bodies. It can also be why someone stumbles on uneven ground or misses a nearby wastebasket when tossing trash. The responsiveness of “proprioceptors” can decline with age, also with injury and neuropathy.
Because proprioception is a relatively new focus of scientific attention, confusion exists about the role it plays in movement—notably in contrast to kinesthesia, usually defined as sensing the movement of the body in space.
Another issue is the relative role of the receptors in thousands of nerve endings in the feet compared with those of proprioceptors located in muscle spindles (also called stretch receptors) that sense changes in muscle length throughout the body.
Proprioception contributes to balance—as do vision and, most importantly, the vestibular system, beginning with movement of fluid in the inner ear. With age comes greater reliance on the visual system, which operates the most slowly—causing people to feel shaky, begin to mistrust their balance and become more sedentary, leading to less use of sensory information and worsening balance.
Also called the sixth sense, proprioception can be the reason that sitting on a hard, straight-backed chair or walking with “minimalist” shoes (thin-soled athletic shoes, aiming to be as close to barefoot as a shoe can be) helps some people with the sensory input they need for better balance and posture.
But ongoing debate rages over the shoe issue: whether minimalist shoes improve proprioception enough to offset the risk of injury due to harder or poorly placed impact with the ground—although structured, cushioned shoes do not appear to prevent injuries. On the other hand, people struggling with imbalance and specific foot problems might need more supportive shoes.
Walking in minimalist shoes has the different advantage of improving foot muscle size and strength, which can help with absorbing impact while running and with preventing injuries like plantar fasciitis and shin splints.
In a Brigham Young and Harvard Medical School study of runners wearing minimalist shoes compared to those doing foot-strengthening exercises and to a control group, the first two groups had similar increases in foot muscle size and strength. But the minimalist-shoe wearers made these gains while at the same time getting in their daily run.
“Both kinds of shoes have some risks associated with them,” writes Mayo Clinic sports medicine specialist Edward Laskowski. For those trying minimalist shoes, introducing them gradually and not wearing them exclusively can help avoid the injuries that occurred when these shoes were introduced.
Exercises to improve proprioception include those involving active movement against pressure, as in weight-bearing activities, and balance exercises done standing on unstable surfaces like an exercise ball.
Most helpful of all, though, can be any activity done “without visual feedback,” such as standing on one foot and walking heel-to-toe along a straight line, as well as any of those done in the proprioception assessment tests.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
DIFFICULTY CONVERTING measurements (500g of rice), estimating the length of a familiar drive and figuring out how much to tip may all stem from a common if unfamiliar learning disorder called dyscalculia.
Compared to dyslexia, dyscalculia—also called math dyslexia—affects almost as many people and plays a role in everything from time management (running out of time or arriving very early) to motor function, such as learning a dance routine.
Under its listing in the DSM-5 under “specific learning disorder,” the explanation “not attributed to intellectual disabilities…” is particularly reassuring for those who mistakenly add zeroes when describing the size of a neighbor’s house or who forget an address immediately after hearing it.
Dyscalculia is increasingly diagnosed in school-age children, affecting 5 to 7% of U.S. students, compared with 5 to 12% for dyslexia. On the other hand, dyslexia research and reports in scientific journals occur nearly 14 times more frequently than dyscalculia.
Even for those considered “good at math” early on, dyscalculia can cause problems, especially once they reach higher-level problems that require manipulating symbols. Having “little creativity with numbers” accompanies uncertainty about solving basic mathematical equations, according to CogniFit.
Many, though, find challenges in “simple mathematical operations,” such as counting backwards, understanding place value and reading analog clocks—and count using their fingers in place of mental calculations.
Difficulties with estimation can interfere with everything from creating a daily schedule to assessing the size of container needed for leftover food or suitcase for a week-long vacation. And problems with spatial awareness can mean hitting your head on furniture when searching for lost objects.
Memory—both short-term and working memory—plays an important role in most calculations. For solving problems, poor working memory interferes with the temporary storage and manipulation of information needed for keeping track of instructions and paying attention.
And poor short-term memory affects keeping track of formulas and tables, such as for multiplication and fractions, as well as of small amounts of information while completing tasks. Dyscalculia overlaps with attention deficit disorder: about 20% of students with ADD also have dyscalculia.
Basic tools to deal with dyscalculia include keeping scratch paper on hand, for example, at meetings to figure out numerical issues as they arise. Another is to post tables and charts where they might be needed, such as common conversion formulas in the kitchen.
For kitchen and office, time management tools like cellphone alarms and timers can help—especially if kept close at hand with phone belts and timers worn around the neck.
Additude offers a free “symptom test” for adult dyscalculia.
CogniFit also offers testing along with a program of “cognitive stimulation”—described as a “series of online therapeutic activities [for] adults with dyscalculia,” based on theories about brain neuroplasticity. These activities are promoted as better tailored for individual profiles than games like sudoku or “brain games” that are touted to improve mental acuity.
(The cost of CogniFit programs, unavailable until you register, is estimated at upwards of $20/month. More importantly, though, research does not yet fully support the beneficial effects of brain games, exercises or activities on neuroplasticity.)
For me, what helped most was simply learning about dyscalculia so that I worry less about my mental functioning when losing track of zeroes in recounting figures or when what looks like a vast expanse of time for running errands turns into a rush. I’ve always known about the need to double-check my numerical reports and for years have relied on an around-the-neck timer for cooking.
What also helped me was that the friend who first told me about experiencing her own dyscalculia is one of the most brilliant and capable women I know.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
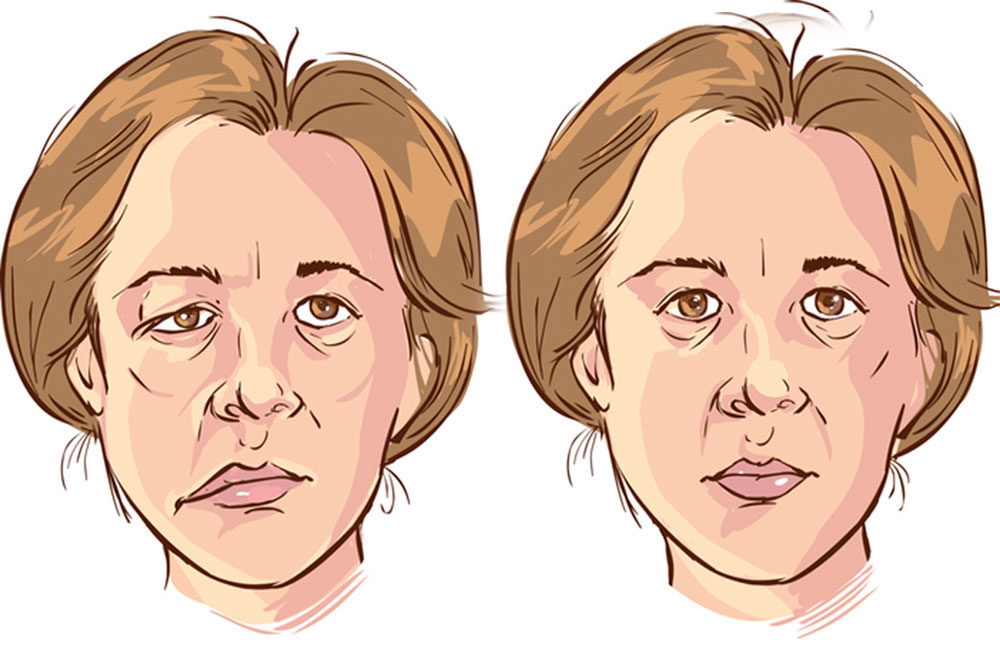
IMAGINE FEELING well enough for daily activities—except that one side of your face droops, involuntarily produces smiles or squints, contracts, or stiffens to the point of becoming immobile and expressionless. You may also drool or shed crocodile tears (tears with no emotional cause).
Sudden drooping or stiffening of one side of the face could be a worrisome early sign of stroke. But a stroke causes muscle weakness in other parts of the body as well, hence the early stroke-detection method FAST that includes raising both arms. Also, a stroke rarely affects the forehead or eye.
Paralysis that arises suddenly, affects only one side of the face and worsens over 48 hours often signals Bell’s Palsy. The condition affects about one in 60 people during their lifetime, and is becoming more prevalent, possibly related to increasing rates of herpes zoster infection.
Incidence of Bell’s palsy increased to almost 40/100,000 during 2000-2010, compared to 25/100,000 in the years 1968-1982. Although Bell’s Palsy is considered idiopathic (no known cause), herpes infection is present in most cases.
Bell’s palsy also arises after infection with the flu or Lyme disease, in pregnant women, and in those with type 2 (usually adult-onset) diabetes. Bell’s palsy is more common between the ages of 15 and 60, with peak incidence around age 40.
Swelling in the facial nerve leads to ischemia, a restriction of blood and oxygen to the nerve cells. What’s also called the 7th cranial nerve has so many functions that any disruption can lead to an array of symptoms that vary from person to person.
Bell’s palsy can include pain (often behind one ear or headache), loss of taste, and hypersensitivity to sound (hyperacusis). Some sufferers cannot close the eye on the affected side, even during sleep. A rare symptom, synkinesis—when facial muscles move in tandem—can cause simultaneous smiling and blinking.
The label “refrigeration palsy” comes from the common memory among sufferers, soon before symptoms begin, of “cooling of the face or a cold draught,” or exposure to cold, such as driving or sleeping with a window open in cold weather.
Bell’s palsy rates were higher during the cold seasons in a two-year study of active-duty military service members, who have a higher incidence of almost 43 cases/100,000, perhaps due to their unlimited access to free health care.
In this group, climate that was both cold and arid appeared to increase risk, although incidence was higher in the southern region of the United States than elsewhere. Also, sufferers spent more time indoors than the “lower-injury group,” leading to the hypothesis that dry indoor air—heated but not humidified—could “traumatize mucus membranes… in turn, induce reactivation of the herpes virus.”
In this study, incidence increased with age—twice as high for those in the oldest group compared with the youngest—and was higher for females than males and married personnel than their unmarried counterparts.
Facial-nerve paralysis dates back at least 4,000 years, based on representations in Egyptian sculptures, and asymmetrical and distorted faces appear in paintings from the Middle Ages and Renaissance. The uneven smile of Mona Lisa’s portrait has been the subject of facial-nerve symposium presentations.
Stress and high blood pressure may play a role in setting off symptoms. During her separation from Brad Pitt in 2017, Angelina Jolie developed Bell’s palsy along with hypertension, and believed sessions of acupuncture helped her recover. Other famous sufferers include George Clooney, Roseanne Barr and Sylvester Stallone.
If stress plays a role in the cause of Bell’s palsy, it is exacerbated for sufferers when symptoms arise and have no clear end point. Most cases resolve within two weeks although some take several months, and 90% recover completely.
Treatment for more serious symptoms can include oral acyclovir starting within three days of the first symptoms, along with steroids to reduce inflammation. And Botox has helped speed recovery from the drooping.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
ON THE MORNING sixty-something development professional C.M. was heading from Philadelphia to Boston for a child’s high school graduation, she woke with a sensation of spinning inside her head. She recognized it from prior experiences: vertigo. If she kept her head propped on pillows and remained still, it wasn’t too bad, but cars and airplanes, standing up and sitting down, would be unbearable.
The spinning that defines vertigo—that the head or the surrounding environment is spinning—is “the perception of motion when no movement is present, or the abnormal perception of motion in response to movement.”
Vertigo is unpleasant and disorienting—and dangerous if you try to drive or climb a ladder. It’s not the same as dizziness—which usually lasts just seconds, while vertigo can persist—or fear of heights, although dizziness can accompany both vertigo and acrophobia.
The most common kind of vertigo is BPV, benign positional vertigo (or BPPV with the added P for paroxysmal, meaning sudden recurrence or intensification of symptoms, such as spasm). Most cases of BPV resolve in a day or two, 80% end within a week; and 95% of patients recover fully.
BPV is usually idiopathic, meaning there’s no known cause, although it occurs more often in those over age 65 and twice as often in women as men. It may be linked to osteoporosis and family history. Lying on the back for a long time, such as in a dentist chair, can be a trigger.
BVP arises from a disturbance in crystals in the ear that monitor the body’s movement. Displacement of the crystals—composed of calcium carbonate and called otolith crystals or otoconia, also debris and “ear rocks”— from the inner ear into the semicircular canals can alter sensitivity to positional changes.
Vertigo can also start with a bacterial infection; an infection that inflames the inner ear (labyrinthitis) or the vestibular nerve (vestibular neuronitis); or Meniere’s disease, causing a buildup of fluid in the inner ear.
Or it can begin in the brain, with migraines or a tumor, or following head injury. Persistent vertigo can be caused by—as well as independently be the cause of—mental health issues, such as depression and anxiety.
The “head impulse test” for vertigo involves trying to hold the gaze on an object (like the doctor’s nose) while moving the head quickly from side to side. When the gaze shifts when moving the head to one side, that can help indicate which ear is affected. Rarely does vertigo affect both.
Indicative of vertigo and thus an aid in diagnosis are unusual eye movements called nystagmus that occur with rapid movement: from sitting to lying down, or with the additional rapid movement of the head to one side and then down (over the side of the bed or other support) below the level of the body.
Vertigo can disappear without treatment when the cause, such as viral infection, clears. Or when the body adapts by relying more on the other senses for balance—either naturally or with the help of vestibular rehabilitation.
To break up the displaced crystals, the series of movements is similar to that used to diagnose BPV. Called the Epley maneuver or canalith repositioning, in which each position is held for 30 seconds after symptoms cease but should be recommended and demonstrated at least initially by a physician.
Depending on the cause of vertigo, antihistamines or medications for seasickness or nausea can help with the discomfort. Because even mild dehydration can trigger BPV, drinking water can help prevent attacks. On the other hand, decreasing fluids via diuretics can help reduce the inflammation that accompanies vestibular vertigo and Meniere’s disease.
Ginger as an all-around nausea-suppressant is on the home remedy list, along with ginkgo biloba, also almonds (perhaps because of their high Vitamin A, B and E content). BPPV can recur, most commonly in people who sleep on the affected side. The best antidote can be adding a pillow under the head and/or using pillows or other props to prevent turning onto that side.
Chronic sufferers should move their bodies, and their heads in particular, slowly when changing position, especially when standing or reaching overhead. In other words, the familiar advice: Move more mindfully.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
PITTSBURGH RETIRED journalist C.S. suffered back pain (following two surgeries to deal with a benign tumor) that made it impossible for her to sit for longer than 20 minutes at a time—and once forced her to lie down flat on the floor in the middle of TJMaxx.
After treatments ranging from traditional physical therapy (PT) to acupuncture, she discovered Myofascial Release (MFR) therapy, which practitioners and patients alike view as an exciting new tool for relieving pain.
Myofascial pain has two sources: skeletal muscles or connective tissues that are ‘”bound down” by tight fascia; and damaged myofascial tissue itself, sometimes at a trigger point where a contraction of muscle fibers has occurred, according to Spinehealth.
The restriction or contraction can inhibit blood flow to the affected structures and heighten sensations of pain.
“Myofascial release means different things to different people,” Virginia Commonwealth University’s sports medicine program director Garry Ho told US News. “But it usually involves applying pressure…to tight muscles and fascia in an effort to get them to ‘release’ and alleviate pain.”
Since the first Fascia Research Congress held at Harvard Medical School in 2007, fascia has been referred to as the Cinderella Story of the anatomy world, according to Runners World: “a major player in every movement and every injury,” that no one paid attention to until recently.
On the other hand, “none of that research is clearly relevant to therapy,” writes editor and former massage therapist Paul Ingraham on PainScience. “Many therapists fascinated by fascia are reaching beyond—way beyond—what the science can actually support.”
“There are lots of theories as to why it works and how it works, but the research is still really murky,” said Ho, noting that most studies on MFR to date have been rejected by reviewers for poor quality and/or bias. A significant problem is the differences among individuals, both in the therapeutic practice of MFR and in the nature of each patient’s pain.
C.S.’s myofascial PT places her hands on various body parts including the back and applies gentle pressure for 10 minutes or so. The therapist also recommends using balls—tennis balls, lacrosse balls and softer balls—that C.S. keeps in her bed to put pressure on areas that become painful.
At the same time, as a complementary therapy, C.S. visits a myofascial masseuse who “uses more motion, gentle as well, but she stretches the fascia with her hands,” C.S. said. Both are “so different from classic PT, and from trigger-point massage that can often be painful.”
But the terminology and practice of each method can vary with individual practitioners. For some, MFR therapy may also be referred to as “myofascial trigger-point therapy.”
And a medical center site compares MFR therapy using sustained, gentle pressure to lengthen connective tissue, without lotions or oils to Swedish massage and deep-tissue massage, which rely on lubricants to prevent friction while kneading and stroking the muscles.
For most of the 400 years since fascia first appeared in anatomy textbooks, surgeons considered it mere packing material to be cut aside before working on the body. In the early 20th century, Ida Rolf’s discoveries that the tissue can become bunched or tangled, or even wrapped the wrong way around organs like the colon, led her to create a method of body manipulation that focused on fascia.
And fascia has long been an important focus of osteopathic medicine.
“As a holistic treatment that looks at the body as an integrated whole, [myofascial release] roots go back a long way, to the soft-tissue manipulations and stretches of osteopathy, which was first done in the nineteenth century.”
While many kinds of professionals—from rolfers and osteopaths to sports medicine doctors—practice MFR, Ho recommends beginning “the cheap way—yourself with tools,” which include foam rollers, a massage cane and massage blocks.
On the other hand, many share the belief that MFR can help people manage pain “mostly because it can help them relax…and there’s a physiological and neurological response to that,” said New York City massage therapist Beret Birkeby.
For C.S., the combination she has put together—MFR therapy and massage, along with her traditional, albeit painful PT—allows her to sit pain-free for long periods and otherwise to regain a “normal” quality of life.”
“Honestly, I think everything has helped, including traditional PT and acupuncture,” she said. “Or maybe nothing helped and the body is just healing on its own time”—exactly why myofascial therapy is so difficult to study but may still be a life-saving answer to pain for many sufferers.
—Mary Carpenter
Well-Being Editor Mary Carpenter reports on news you can use right here every Tuesday.
ARLINGTON BIBLICAL scholar D.T. noticed a surprising after-effect of the light anesthetic she received for orthopedic surgery: the depression she’d been fighting for years with an array of medications, which had worsened recently, started to lift.
The anesthetic: ketamine, used in orthopedic surgery because it can reduce post-operative pain, is in the class of drugs known as dissociative anesthetics that includes PCP and nitrous oxide.
Because most adults don’t like the feelings of detachment and hallucinations ketamine can cause, it is most commonly given in pediatric surgery. Kids seem not to notice what D.T. calls the “trippy” effects.
Starting about 20 years ago, low-dose (subanesthetic) ketamine given to patients for chronic pain appeared to allay their depression. Chronic pain and depression are often “inextricably intertwined,” with treatments including antidepressants and electroconvulsive therapy (ECT) effective against both.
But it turned out that patients suffering treatment-resistant depression without other physical or psychiatric illness also benefited from ketamine.
“Night and day,” was how D.T. described the difference. “Post-op I felt like a normal person for the first time in years.” Compared to SSRI medications (e.g., Zoloft and Prozac) that take weeks to work, she said, “ketamine, one dose, and bam, [I felt] totally different.”
In the past few years, clinics offering ketamine infusions for mood disorders have multiplied around the country. Actify Neurotherapies, which oversees ten clinics including the Potomac location that D.T. uses, received 28,000 inquiries in the first nine months of 2018.
And this March, the FDA approved the first ketamine-based drug to treat depression, although its reception was tepid. Because esketamine is a nasal spray, some worry about uncertainty of the dose —like D.T., who points out that worries could affect attitude, which plays an important role in the ketamine experience.
Ketamine doses for “treatment-resistant depression”—defined as major depression that hasn’t responded to two or more medications—range from 40 to 80 milligrams per kilogram of body weight. That’s about one-tenth the amount used recreationally in the drug known as “special K.” (Higher ketamine doses are used for anesthesia as well as for veterinary euthanasia.)
Ketamine’s mood-enhancing effects emerge in about four hours—providing a quick “window of relief,” especially for patients who might be contemplating suicide. Rapid reduction of suicidal thoughts can allow time for sufferers to get more in-depth treatment. That “window” can also demonstrate to those with intractable mood disorders that something exists to help them.
Unusually for a mood-disorder drug, ketamine appears to help with both depression and anxiety—two diagnoses traditionally viewed as distinct but increasingly seen for their overlapping symptoms, such as problems with sleep and fatigue, irritability and difficulty concentrating.
“Some people react with anxiety to life stressors—and some people, in addition, go beyond that to become depressed,” said David Barlow, director of the Center for Anxiety and Related Disorders at Boston University.
The effects of ketamine can be different for each diagnosis: for depression lasting one to two weeks and, for anxiety, more than two months—although individual reactions can vary.
Ketamine may work by increasing the neurotransmitter glutamate, which appears to help neurons communicate with each other along new pathways and facilitate communication among specific areas in the brain—known as neuro-connectivity.
“There is no ‘I,’ time disappears, you are released from negative inner emotions like anger, and you can surrender,” Gabor Maté, a Canadian physician specializing in childhood trauma and psychedelic-based therapy, told a recent Psychotherapy Networker conference in D.C.
“You feel less separate from the rest of the universe, part of the plasma,” D.T. said.” “You feel more alive.”
Visually, ketamine often creates bright colors and images—called “visions” (rather than hallucinations that can be hard to distinguish from reality). D.T. compared her experience to a dream: “You know that you can open your eyes any time and see what’s really there.”
With her eyes closed, she has been “out west; in a baroque-styled room; and in a video chasing something.” But for her, the strongest sensory effects were auditory: “I was inside the piano.” For people embarking on ketamine therapy, she “strongly suggests they bring music that makes them feel happy.”
To allow for slow increases in dose as needed, the Actify protocol begins with a series of five infusions given over a three-week period, D.T. explained. Before and after each infusion, patients speak with a doctor; and afterwards they fill out questionnaires on depression and anxiety. During the hour or so of each infusion, medical professionals check bloodpressure and general well-being. The entire appointment lasts about three hours.
After taking two antidepressants “for years,” on the advice of her psychiatrist D.T. stopped both within months after starting ketamine—a big financial savings to her, she noted. Each ketamine infusion at Actify costs just under $500 (not covered by insurance).
After more than 12 infusions altogether over little more than a year, D.T. has had no physical side effects, which is true for most who have tried the therapy. If there’s a downside, she said, it’s heightened sensory sensitivity so that, for example, “the mall is too much.” Side effects, which occur more often among those who regularly take recreational doses, can include bladder issues such as cystitis.
On the other hand, patients can develop tolerance to therapeutic ketamine, requiring ever-higher doses—making the drug potentially addictive. But D.T. has been requesting lower doses, saying, “I want to see how low I can go and still feel better afterwards.”
An investigation by STAT News found wide-ranging inconsistencies among the clinics—with a number straying from recommendations issued last year by the American Psychiatric Association. While some like Actify have psychiatrists on staff to do intake checks at each infusion, many had no mental-health professionals.
The clinics surveyed charged anywhere from $350 to close to $1,000/infusion. And many overhyped the treatment, which can help 70 to 85% of patients, but effects vary among individuals.
When it works, ketamine provides another step before the final, more drastic option of ECT. While ECT has been modified over the years and is considered very effective against depression, it can have serious side effects, notably memory loss.
And compared to SSRI medication, D.T. points out, “ketamine’s success would be much better even if it helped only 50%.”
—Mary Carpenter
Well-Being Editor Mary Carpenter reports on news you can use right here every Tuesday.
“FIBERS IN a variety of colors protrude out of my skin like mushrooms,” said Joni Mitchell about her Morgellons disease, which has left her housebound and feeling as if she’s being “eaten alive.”
Morgellons disease (MD) is a “disfiguring and distressing condition,” according to dermatology researchers at Wake Forest. Symptoms include sensations of crawling, biting and stinging on the skin that can be very painful; and multiple, non-healing skin wounds.
But the existence of red, blue, black and white fibers in the skin is the most notable complaint— hence the nickname “fiber disease.” Patients bring scabs and other skin samples with embedded fibers—called “matchbox” or specimen signs —for testing.
Until recently, most of the medical community agreed with the CDC conclusion that Morgellons symptoms are based on “delusional parasitosis,” a psychiatric condition in which sufferers erroneously believe bugs are infesting their skin. (Ekbom Syndrome is a related form of delusional parasitosis.)
The CDC analysis of 115 patients determined that the protruding fibers were made of cotton—not bodily substances—and traced the skin sores to “long-term picking and scratching the skin.”
Noting that symptoms of Morgellons are similar to those of Lyme disease (LD)—fatigue, itching, joint aches, loss of short-term memory, difficulty concentrating, insomnia—the CDC tested for and eliminated Lyme. Morgellons researchers at Oklahoma State University agreed that “there is no evidence” linking MD to the spirochetes that cause Lyme.
“Borrelia spirochetes are readily detectable in MD tissue, but sensitive and specific methods are required,” assert Canadian microbiologist Marianne Middelveen and colleagues. “The CDC used “two-tier serological LD testing…although specific for Bbss, lacks sensitivity and is little better than a coin toss in detecting LD.”
In addition, Middelveen and colleagues write that MRI imaging shows alterations in gray matter than could be linked to spirochetal infection. And that careful sectioning and staining of skin samples “determine the keratin and collagen nature of these fibers.”
Linking these fibers to Lyme, they suggest that “underlying spirochetal infection causes a filamentous dermopathy that is accompanied by an array of LD-like multisystem symptoms.”
In the researchers’ paper, “History of Morgellons disease: from delusion to definition,” they point out that the CDC conclusions did not meet conditions for the diagnosis of delusional disorder based on the DSM 5 — the diagnostic manual for psychiatric conditions —notably that any possible physical cause must be excluded.
“In most of the case studies that equate MD with [delusional disorders]… evidence of disease (physical and laboratory) was dismissed, fibers were identified as being textile in origin based solely on visual examination, physicians were unwilling to examine skin at sufficient magnification to see microscopic fibers,” they write.
Delusional disorders share overlapping symptoms with other diagnoses—notably the “overvalued ideas” present in OCD, body dysmorphic disorder, hypochondriasis. But while OCD often involves mistaken ideas, for example about cleanliness, that diagnosis requires repetitive, ritualistic behaviors that are absent in delusional disorders.
Delusions in one sub-category, “somatic” (referring to bodily function or sensation) range from the “bizarre,” such as that one’s bones are twisted around each other; to non-bizarre, which “mirror real health conditions,” such as broken bones.
Among non-bizarre delusions are partial paralysis, bodily odors and pregnancy. Reported cases include a man who complained that he was unable to sleep at night, despite tests showing he slept for many hours; and a woman who could feel a foreign substance in her mouth that interfered with eating, although no such substance could be found.
What can make Morgellons most challenging for sufferers is lack of awareness of the condition, even among doctors. “Unexpectedly getting a psychiatric diagnosis when you believe you have a skin disease can be devastating,” writes Nancy Moyer on Healthline and can, in turn, “worsen symptoms or even lead to new ones.”
Defining MD as a psychiatric condition gains support from the occasional positive response of symptoms to antipsychotic drugs, which target the neurotransmitters dopamine and serotonin. On the other hand, “reduced growth of parasites and anti-pruritic properties” are listed as off-label effects of these medications, according to Middelveen.
Treatment for Morgellons often includes psychological approaches, such as cognitive behavior therapy. But because the belief of MD sufferers that they have a physical disease is so difficult to dislodge, many are resistant to or upset by such recommendations.
One cause of delusional parasitosis is recreational drug use—with “coke bugs” and “meth mites.” In a study of 147 patients complaining of bug infestation, 11% had a history of drug use (methamphetamines, cocaine, heroin, marijuana, and other street drugs), according to Middelveen.
Among MD sufferers, Joni Mitchell admitted to “taking a lot of drugs over the years, including mounds of coke,” according to the Daily Mail. But she was also a victim of childhood polio, a potential infectious link for MD that has not yet been pursued.
—Mary Carpenter
For more reporting from well-being editor Mary Carpenter, click here.
THE BEST protection against the sun’s harmful UV rays would require staying indoors or in the shade during the brightest midday hours. But on occasions when that’s impossible, such as wishing to swim when the weather app says 40% chance of thunderstorms all day, any break in the clouds means you’ve got to go.
Water magnifies the burning effects of the sun and can disable some of the best sun-protection formulations. While all sunscreens should be reapplied every two hours, the SPF can drop by as much as 50% after just 40 minutes in water and possibly faster in salt water.
Sunscreens labeled waterproof (technically “water-resistant”) should offer at least 80 minutes of protection. For non-swimmers, water-resistant sunscreens last longer in sweaty weather.
Choosing the best sunscreen for any occasion is always a trade-off between two kinds of barriers—with two categories of ingredients: the physical, or mineral, uses zinc oxide and titanium dioxide; the chemical includes avobenzone, oxybenzone, octinoxate and octisalate.
Sunscreens that create physical barriers on the skin’s surface begin to work immediately but also wash off more quickly, with most products listing endurance at 40 minutes. Zinc oxide may offer better protection than titanium dioxide, but for those who recall the white noses of tennis players and skiers in the old days, high zinc concentrations at the “paste” level these days are sold only for use on horses’ heels.
“None of the mineral sunscreens in our tests this year did well enough to make our list of recommendations” is the latest conclusion from Consumer Reports.
Chemical sunscreens, because they must be absorbed by the skin to work, require application 15-30 minutes before needed but can last up to 80 minutes in water. Based on the math, they offer longer protection but only with advance planning.
On the other hand, many of these chemicals harm the environment, notably coral reefs, and possibly their users as well. Based on recent human health-related findings, the FDA is expected to propose “big changes to sunscreen regulations” in late 2019, which might obviate the selection process entirely.
While using both physical and chemical sunscreen at the same time might seem like a good way to get the benefits of each, such a combination risks diluting or even canceling out the protection offered by either one.
As for SPF, experts disagree: Some assert little benefit in any SPF over 30, while others recommend the highest number possible (100+) for longest-lasting as well as highest-level protection.
According to Consumer Reports, “no sunscreen blocks 100 percent of UVA or UVB rays. The breakdown: SPF 30 blocks 97 percent of UVB rays, SPF 50 blocks 98 percent, and SPF 100 blocks 99 percent.”
Also from Consumer Reports: “The SPF number gives you no information on how well a sunscreen protects against UVA rays. That’s why you need to look for a broad-spectrum sunscreen, which protect against both UVA and UVB.”
Based on the discovery that the true SPF of many products is lower than listed, Consumer Reports notes that choosing “a sunscreen with chemical active ingredients and an SPF of 40 or higher will give you a better chance of getting at least an SPF 30.” Dermatologists surveyed by Prevention Magazine suggest SPF 50 and higher.
Achieving the posted SPF requires heavy application—some say a shot-glass worth over the whole body. Lotions can be applied more evenly and generously, while sprays make it harder to reach sufficient SPF. And sunscreen included in moisturizers is too diluted to offer much protection.
An additional concern is the pore-blocking or comedogenic properties of different sunscreens. Maryland editor C.M. and her daughters —a self-described acne-prone family—have sampled many options only to agree: “there is no such thing as non-comedogenic.” They also deem avobenzone “the worst offender” among sunscreen ingredients for leaving yellow stains on white clothes.
In the end, though, dermatologists and others observe that everybody’s skin is different, and some do better with unlikely formulations—which refers the testing and selecting back to the individual.
Once the choice has been made, expiration dates are important. Products not stored in a cool, dry place can become less effective before the printed end-date. Also, shake before using to make sure the sun-protecting ingredients are spread throughout.
Only Lifejacketadvisor gives recommendations for the best water-resistant sunscreens (all for 80 minutes): for physical barriers, Blue Lizard Australian SPF 30 as “simply the best water-resistant,” and EltaMD UV Sport SPF 50; and for chemical formulations, Neutrogena Beach Defense SPF 70.
The only general sunscreen review to include “best water-resistant” (also 80 minutes) named Sunology Mineral Sunscreen SPF 50.
While sunscreen reviews differ almost entirely on their top pick, the one overlap goes to EltaMD UV Broad-Spectrum SPF 46 (physical), winning “best overall sunscreen” on New York Magazines’s Strategist as well as from dermatologists polled by Prevention Magazine.
When choosing sunscreens, don’t forget the lips. To be avoided: lip gloss, which can attract UV rays; ingredients like menthol and camphor, which can be drying and irritating; and beeswax, which can cause an allergic reaction. Winners from reviewers: EltaMD SPF 31 and Vanicream Lip Protectant SPF 30—both physical; and for chemical, Banana Boat Sport Performance Lip Balm SPF 50.
Best known for protection against jellyfish, the whole-body suit is a completely different kind of physical barrier, made of synthetic materials, including nylon, and effective against sunburn as well.
For the face alone, some prefer wearing a swim mask with snorkel. Or a balaclava — made of synthetic material like the jellyfish suit with a mask-sized opening—protects the entire head and neck as well.
A similar, newer option with tiny separate slits for the eyes, nose and mouth—although some complain about trouble breathing—is the “facekini.” In the end, though, there’s the Consumer Reports conclusion: “Research shows that people who rely on sunscreens alone tend to burn more than those who stay in the shade and wear long sleeves.”
—Mary Carpenter
Well-Being Editor Mary Carpenter reports on news you can use right here every Tuesday.
BREAKING A kneecap sounds like an excruciatingly painful injury, the result of a dramatic accident in which the knee slams against a hard surface like concrete —and it almost always is.
When Maryland graphic artist S. H. tripped over a table in a crowded room and landed on a hardwood floor, she knew she needed to go to the ER. There, she rated her pain level 9 out of 10. The treatment: a hip-to-ankle “immobilizer” on her leg around the clock for a month, no walking and no driving; and after that, wearing the immobilizer most of the time, with driving and some walking, until the break heals—typically eight to twelve weeks altogether.
But in my case, after falling lightly on a rocky trail, I felt fine walking another three miles, going to the grocery store and afterwards following the RICE (rest, elevation, compression and ice) formula for four days until I could get an orthopedic appointment. After the x-ray, my doctor said there was a fracture, but because I’d been walking on it, I could skip the immobilizer and move directly to a soft brace, with weekly x-rays to check on healing.
Based on this experience, patellar (kneecap) fractures can be more worrying than they feel or appear. The fact that they “can lead to profound impairment” is countered by the anodyne-sounding description of most as a “simple two-part diversion caused by a direct blow (i.e. dashboard injury)”—almost 80% are the result of traffic accidents. Most common between ages 20 to 50, these fractures are twice as likely to occur in men.
Patellar fractures comprise a “broad range of subtypes,” notably “non-displaced”—cracked or broken but still in the correct place (the kind S.H and I had) —or “displaced,” with parts of the bone out of place that require surgical repair using screws and ties. (In the worst cases, almost 7%, “open fractures” involve broken skin, require more complicated treatment and can result in “devastating soft tissue conditions.”)
The patella measures about two square inches in an ovaline shape, like a fig with the stem end facing downwards where the bone attaches to a ligament. The patella is the body’s largest sesamoid (derived from the Latin for “sesame seed,” because most are small) bone—by definition embedded in a tendon or muscle, in this case the quadriceps.
There it acts like a pulley by creating a smooth surface that increases the muscles’ ability to transmit force and extend the knee. It makes the muscles more efficient and absorbs stress between the upper and lower portions of the leg.
A clue to kneecap injury is difficulty bending the knee—as in walking downstairs. In addition, touch can often reveal a break, especially soon after the injury before the knee starts to swell. The “straight-leg test” —holding the leg straight and trying to raise it while lying flat —can help determine if the tendons or the patella are “disrupted.” The x-ray is definitive.
The degree of injury can depend on the amount of damage to surrounding muscles and tendons. Long-term knee problems following patellar fractures arise most often from disruption of the cartilage on the underside of the kneecap, with increased risk linked to preexisting arthritis in the knee.
Healing requires weeks of patience as well as intense mindfulness with every step. Especially when heading downstairs, I must remind myself —counterintuitively —to lead with the damaged leg. Besides working on extension, the patella also creates resistance to decelerate knee flexion. When walking downstairs or downhill, the patella must withstand force equal to four or five times your body weight during the moment when the other leg is suspended on its downward swing.
The most oft-repeated advice is “You need to be especially careful now, so don’t fall.” In my case, I had written, just the week before, about the relief of feeling generally braver after a session of falling practice.
In my post, I tried to be clear that whatever moves you’ve practiced, the moment of a fall is often too quick to put them to work. Although the narrow, rock-strewn path where I fell offered few options for safe falling, I remember having a one-second flash about doing something different to prevent injury.
Now I’m worried about falling in an entirely new context—of protecting the injured knee—along with being more superstitious than ever about what I write or say.
But my conclusion stands: “For the occasions when I still find myself trying to do more than one thing at a time, I know what I should really be practicing is not falling, but strength and balance—and maybe most important, mindfulness.”
—Mary Carpenter
Well-Being Editor Mary Carpenter is more determined than ever to practice mindfulness. Read more of her posts right here.
AT URBAN EVOLUTION in Alexandria, I fell down about 30 times in a row—forwards and backwards; to the left and then to the right—and felt much better by the end. Early on, I became slightly breathless—not from the exertion but from apprehension—which diminished over the course of my hour-long session.
The main business of Urban Evolution is Parkour, “a free-running acrobatic sport” that involves leaping off obstacles and includes learning how to land. Geared to ages 35 and over, its “401 PK (Parkour)” classes aim to develop the balance, strength, flexibility and mobility involved in “bailing”—falling in Parkour language.
Parkour emphasizes resilience and flexibility—exactly what tends to decline with age. Parkour is “strengthening, having fun with movement and adapting to the environment,” Boston Parkour coach Blake Evitt told Mother Nature Network, which cites Parkour as a “workout that emphasizes how to fall safely.”
Whether learning and practicing good ways of falling can help in that split second when you fall, no one knows until it happens to them. But although practice could help, the more certain achievement of my session was feeling braver.
My fearfulness surprised me, although I’d noticed becoming more apprehensive and cautious with passing years. That’s what drove me to take the $60 private session, rather than a class, with Urban Evolution’s founder and owner, Salil Maniktahla. I wanted to be sure someone watched me all the time.
Fear of falling can restrict activity—and less activity can lead to declining balance and muscle strength, which increases the risk of falling, according to Kathy Cameron, director of the Falls Prevention Resource Center at the National Council on Aging (NCOA).
Incidence of falling is highest among 50- to 60-year olds—“more than older folks,” writes Michael Zimmerman in the AARP magazine. “We’re more active, and that puts us more at risk of falling.”
Falling is the most likely cause of traumatic brain injury (TBI), according to the CDC. And among U.S. residents age 65 and up, “about 20% of those who fall have an injury like TBI or a hip fracture or other broken bones,” Cameron told CNN.
The reason for most falls: people trying to do too much at once “without being attentive,” according to Toulouse University Hospital physician Antoine Piau, lead author on a study that reviewed 371 falls reported over a four-year period.
“Falls happen where people spend most of their time,” said Kaiser Permanente physician Eric Larson in Seattle. They fall when they get up in the night to go to the bathroom—often in bare feet on slippery floors. In the study, people fell most often at home and often in the bedroom, while only 2% of falls happened on stairways.
Four out of five falls occurred in well-lit areas; almost two-thirds, slips or trips; and almost 90%, because people lost their balance. Injuries requiring medical attention occurred in 119 of the falls, and 19 resulted in reduced walking ability.
In addition to practice falling, the other element involved in staying safe is prevention. The 15 “Falls Prevention Programs” on NCOA’s list are mostly designed for people unable to practice actual falling because of physical limitations or phobias. In fact, the search for programs that address falling most often directs you to programs for “seniors.” (The NCOA list of Washington, D.C.-area programs begins with Iona Senior Services and Geriatric Care Counselling.)
NCOA programs, such as “A Matter of Balance,” are designed for those not currently participating in regular activity, Sara Pappa, coordinator for Northern Virginia Falls Prevention Alliance, told MyLittleBird. Many include lectures, for example, on rearranging the environment (notably eliminating area rugs, which are a frequent cause of slipping and forbidden in most senior communities).
At the next level, SAIL (Stay Active and Independent for Life) involves hour-long aerobics classes of evidence-based strength and balance exercises—most done standing, Pappa noted: “Standing on one foot and moving the other forwards, to the side and back; walking toe to heel forwards and backwards; and walking in a circle with arms out to the side.” Ankle weights can be added. One goal is “to help you think about where you are in space,” she said.
Although not unlike the balance exercises that began my Parkour session, the repeated practice of actual falling has the benefit of lessening fear, which in turn can help avoid the instinctive reaction of tensing during a fall, the reaction most likely to cause injury.
For safer falling, the key is to lower your center of gravity, Salil explained. Get as close to the ground as possible by bending knees, crouching and curling while falling.
In a “four-point plan for safe crash landing” from stuntwoman Alexa Marcigliano (“Orange is the New Black” and “Blindspot”) cited by Zimmerman, the first rule is stay bent.
The others are protect your head by turning it to the side or tucking your chin; “land on the meat” —thighs and upper arms instead of bony parts like elbows; and keep falling—instead of bracing to stop, continue to roll, which spreads the impact across a larger surface of your body.
Marcigliano talks about “slapping out.” As you fall, extend arms forward, elbows bent, with flat palms—which can absorb a lot of weight—actually slapping the ground. Practicing this move came early in my session with Salil.
Near the end he addressed my most frequent worry: slipping and falling backwards on uneven downhill surfaces with dry, loose dirt and pebbles in Rock Creek Park. For me, practicing backwards falling was the scariest but also the most elating.
Salil recommended watching videos of “Parkour ukemi,” loosely translated as “the art of falling” in the context of Parkour.
Parkour ukemi videos portray all levels—from older women in harnesses tripping on uneven or treadmill surfaces to unimaginably acrobatic moves by Parkour experts.
Although I left Urban Evolution pleased with my successful falls, the truth is that I spent most of the time on a very thick, bouncy mat, with a few falls on the next harder surface—but still many levels away from real-life sidewalks or even Rock Creek Park trails.
My “homework” included calf-raises—getting up on tiptoes, first on both feet, then on one at a time; and hops using both feet, forward and backwards, then side to side.
Push-ups to increase strength were also on the list. For people unable—or never able, like me—to do these, Salil recommends slow “push-up negatives” that include only the downward movement and can involve flopping down the last several inches.
When I asked about practice falls on grass, maybe with a towel, Salil looked worried. Instead he suggested, diplomatically, using a large, thick blanket, but he warned: “Be very careful!”
For the occasions when I still find myself trying to do more than one thing at a time, I know what I should really be practicing is not falling, but strength and balance—and maybe most important, mindfulness.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
IN HIGH school, my “big sister” Kate drowned in a swimming pool. I knew Kate had epilepsy—sufferers are almost 20 times more likely to drown (if a seizure occurs while swimming) than the rest of the population.
Epilepsy recently became the first condition for which a CBD-based treatment won FDA approval, though only for two rare, difficult-to-treat forms of the disease. But how CBD alleviates symptoms of epilepsy remains a mystery as do many aspects of the disease itself.
Epilepsy’s definition sounds straightforward: a central nervous system (neurological) disorder in which brain activity becomes abnormal, causing seizures or periods of unusual behavior, sensations and sometimes loss of awareness.
But the disease is not simple. Symptoms can be very different depending on which part of the brain is affected; in about half of sufferers, treatment medications are ineffective or only partially effective, and the cause of their epilepsy is unknown.
In the case of my college friend Pam’s “frontal-lobe epilepsy,” symptoms like grimacing and screaming got her labeled “crazy” by family and friends. “Temporal-lobe epilepsy,” the diagnosis in a recent Washington Post medical mystery, can cause buzzing sensations throughout the body as well as feelings of terror and detachment. Both are ““epilepsy syndromes”, characterized by specific clusters of features involved, such as the part of the brain affected, the cause of the seizures and the age at which they started.
Most anti-seizure drugs work by slowing down excitatory nerve activity in the brain. But debilitating side-effects, such as fatigue, headache, dizziness and vertigo, vomiting and liver damage, can drive sufferers to reject the drugs. When people said about my big sister, “Kate didn’t take her medication,” we heard blame as we did for my friend Pam’s unhinged behavior.
In addition to blaming sufferers, most people have no idea how to react to someone having a seizure, and traditional wisdom is generally wrong. The worst response is putting something in the mouth. Although there’s no risk of sufferers swallowing their tongue, stiffening muscles may tighten during a seizure, causing the person to bite down. If something is in the person’s mouth, they may swallow the object or break their teeth.
Restraining someone having a seizure can make them confused, and in some cases, aggressive. And “rescue breathing” is generally unnecessary and risks injury.
Instead, what’s important is timing the seizure to determine whether medical help is needed. While most seizures last only a few seconds or minutes, some that begin with minor symptoms get worse. If a seizure lasts more than five minutes or causes difficulty breathing, call 911.
Besides timing, reassure the person and keep them safe. Make them comfortable by loosening tight clothes; help them lie down if there’s any risk of falling; and especially if someone is unconscious, turn them on their side with their mouth pointing toward the ground to ease breathing.
For about half of sufferers, epilepsy can be traced to a specific cause such as genetic influence; head trauma; brain conditions such as tumors or stroke; and infectious diseases such as meningitis.
Although symptoms appear throughout the body, the electrical events responsible for epilepsy always occur in the brain. Focal (partial) seizures affect only one area of the brain and often don’t cause loss of consciousness. Generalized seizures, what people used to call “epileptic fits,” involve the whole brain.
Among types of generalized seizures, “absence seizures” may include brief loss of awareness. The other types affect the muscles: tonic (stiffening); atonic (loss of muscle control), clonic (repeated, jerking muscle movements) and myoclonic (brief jerks or twitches of the arms and legs).
The sixth and most dramatic kind, tonic-clonic seizures—previously called “grand mal” —can cause abrupt loss of consciousness, body stiffening and shaking, and sometimes loss of bladder control.
The greatest risk for sufferers of epilepsy is known as SUDEP (sudden unexpected death in epilepsy) that can be linked to no other cause and most often occurs during sleep.
Medications to treat epilepsy, which have increased two-fold over the past ten years, help control seizures for most of the three million Americans with epilepsy—but only when sufferers get the right drug for their particular epilepsy syndrome, which many physicians are still unable to recognize.
Other treatments involve nerve stimulation, using devices that are implanted or placed on the skull. An implantable vagus nerve stimulator has reduced seizures in about a quarter of patients receiving the treatment.
Surgery used to be considered a last resort, but it may also work well in the early stages of temporal-lobe epilepsy. Removing the temporal lobe can stop seizures almost completely in about 60% of sufferers who have the procedure —results that occur in less than 10% of those taking medication alone—and therefore, can be a “true cure” for the disease.
As for CBD, the medication Epidiolex has fewer side effects than traditional epilepsy drugs, although high doses can cause fatigue, diarrhea and liver damage. In one study group, those taking 10 mg had 37% fewer seizures—compared to a 42% reduction in those taking 20 mg—but the lower dose produced fewer side effects and was thus preferable.
Capitalizing on the momentum of Epidiolex approval, researchers are looking into sources of CBD other than the strictly regulated cannabis plants, such as synthetic CBD and CBD produced by “yeast factories” (using a network of enzymes that turn sugar into cannabinoids). These produce a purer, cheaper product and avoid the high water and energy demands that cannabis cultivation makes on the environment.
—Mary Carpenter
Every Tuesday, well-being editor Mary Carpenter reports on health news you can use.
WHEN I walked into a recent board meeting, I spotted a relatively new member whose name I didn’t remember. But while going through the alphabet—my customary mnemonic device—I tripped on the carpet.
The best antidote to forgetting and to falling, in addition to many stress-related health issues? It may be mindfulness, but only when calm and focused attention becomes habitual.
One testament to the numbers of people searching and willing to pay good money to become more mindful is a recent kickstarter campaign for the “Moment Pebble,” a small lighted rock that dims and brightens to guide breathing during a 30-second period.
By last month, the Pebble had raised $74,000 from U.S. backers and thousands more pounds from its British fans on Kickstarter, where about $50 (converted from pounds) secured one Pebble to be delivered in September. In the ongoing effort on Indiegogo, one Pebble requires $51; the selling price after the official market launch will be around $75.
Although it sounds silly and pricey, the pebble’s glowing light promises to focus the mind and slow the breath, the two most important components of mindfulness meditation. In this type of meditation, “you focus on being intensely aware of what you’re sensing and feeling in the moment, without interpretation or judgment…engaging your senses outdoors is especially beneficial.”
While daily meditation sessions can increase focus and calm, it can be most difficult to employ mindfulness at exactly those hectic times when risks of forgetting and falling—and of long-term health effects from stress hormones coursing through the body—are the greatest and most worrisome.
From the outset, developing a mindful meditation practice usually requires serious, personal and in-depth training.
For DC artist A.M., a 90-minute session at The Mindfulness Center (TMC) in Bethesda made the difference. Therapist Aurora Hutchinson listened to A.M.’s problems—debilitating head pain concentrated in her jaw that persisted following a concussion —and worked with her to teach and practice relaxation and meditation techniques tailored to her needs.
In her standard 60-minute “Stress Reduction and Lifestyle Counseling” sessions, Hutchinson uses mindfulness meditation to improve overall health and to help with issues like navigating transitions, prioritizing and finding motivation, according to TMC’s Jessie Taylor.
A more intensive training, the eight-week “Mindfulness-Based Stress Reduction” (MBSR) course, has helped many thousands of people since its creation by Jon Kabat-Zinn at the University of Massachusetts, Amherst, in 1979. (It’s offered locally by the Insight Meditation Community of Washington.)
I had tried learning mindfulness on my own using the MBSR workbook and CD, but it took the course’s weekly meetings, along with daily practice using the five-to-45-minute CD-guided-meditations for me to ratchet down my stress levels. The $500 class fee provided extra motivation.
Spending 10-15 minutes attending to my in-breath and out-breath has become an effective, efficient way to calm my mind —even on the most stressful days— but it also affects my body and usually puts me to sleep. Despite the positive nap effect, I miss out on practicing focus and attention.
Many in the mindfulness community are opposed to gadgets. Richard Davidson, founder of the Center for Healthy Minds at the University of Wisconsin-Madison and a “dedicated meditator,” points out that meditation in Sanskrit means “familiarization,” referring to one’s increasing familiarity with the nature of one’s own mind. Focusing on external signals can be a distraction from learning about ourselves and becoming more effective meditators.
Most mindfulness-improvement gadgets cost more than $100, most respond to and track stress levels, and most are worn on the body. The Muse includes a large sensor band placed on the forehead; the Thync sends the appropriate vibrations to pressure points behind the ears when it senses the need for boosting energy or calmness.
The “Spire”—also described as Pebble-like—measures breathing and guides breathing exercises when needed.
The Phi, another hand-held device, tracks calm and focus and offers both real-time alerts of stressful breathing and an interactive multisensory experience, stimulating all the senses except taste.
Compared to other gadgets, the Moment Pebble activates only when the user chooses (no feedback or tracking) to provide 30 seconds of mindfulness practice. And because the Pebble’s dimming and brightening light guides the breath, a user’s eyes must stay open—no falling asleep —until the final pulse of bright light indicates “the end of your moment.” Though paying for a pebble still sounds silly, the Moment Pebble might offer the help I need.
—Mary Carpenter
Every Tuesday in this space, well-being editor Mary Carpenter reports on health news you can use.
“YOU SHOULD never call a psychopath a psychopath. It upsets them.” That’s a favorite quote from the charming, murderous Villanelle in the TV series “Killing Eve.”
Both Villanelle and real-life Theranos founder Elizabeth Holmes, profiled in John Carreyrou’s book Bad Blood and in a Jennifer Lawrence-starring film in the works, have been called psychopaths. Psychopathy is not an official diagnosis but instead encompasses extreme forms of several personality disorders, notably antisocial personality disorder (APD) and often narcissistic personality disorder (NPD).
The 10 personality disorders, which are grouped into three clusters in the DSM 5 (the diagnostic manual for psychological illnesses), “denote rigid, inflexible and maladaptive patterns of thinking and behaving leading to impairment in functioning and/or significant internal distress.” About 30% of people requiring mental health treatment have at least one personality disorder.
Cluster B disorders are “characterized by dramatic, overly emotional or unpredictable thinking or behavior.” Along with APD and NPD, Cluster B includes histrionic personality disorder (HPD) and borderline personality disorder (BPD). Grandiosity, the need for admiration and a callous lack of empathy are characteristics of all four.
(Cluster A is characterized by odd, eccentric thinking or behavior, including paranoid and schizoid disorders; Cluster C is characterized by anxious, fearful thinking and behavior, including obsessive compulsive disorder [OCD].)
While each personality disorder is viewed as a distinct mental illness serious enough to create problems relating to other people, many overlap. Among people with BPD, for example, 85% meet the diagnostic criteria for at least one other personality or mood disorder.
“People with antisocial personality disorder are willing to use deception or manipulation to get what they want… show no regret or guilt…lack a sense of empathy and cannot consider the feelings of others without help,” writes Kathleen Smith on Psycom.
But high-functioning people, who are charismatic and successfully hold positions of power, are “not the norm” with APD. Also labeled sociopaths, they struggle with irritability and aggression and tend to behave impulsively and irresponsibly.
Elizabeth Holmes convinced investors like Henry Kissinger and Betsy DeVos to hand over some $600 million for her seemingly miraculous finger-prick home blood test before being exposed as a fraud. She created an intimidating persona,based on her hero Steve Jobs. She wore all black and lowered her voice to a “mesmerizing deep baritone,” according to Carreyrou—although that tended to slip after a few drinks.
Despite Holmes’s “unflinching” blue-eyed stare, the myth about psychopaths never blinking isn’t true. Some blink very little at photos that are disturbing or unpleasant, but most blink often when lying.
Holmes acted with grandiosity and self-importance, and she fired employees ruthlessly—all typical of those with NPD. Her wealth once estimated at $4.5 billion, Holmes now faces up to 20 years in prison.
Which personality disorder is most prevalent has changed over the years, according to several studies. OCD held the top slot in 2008, APD in 2002 and HPD (characterized by “constant attention seeking, emotional overreaction and seductive behavior…tend to overdramatize situations, easily susceptible to the influence of others”) in 1997.
Louise Turpin, the California woman who has been accused along with her husband of starving, torturing and imprisoning their 13 children, received this diagnosis, though not the hoped-for release from jail to a mental health treatment center while awaiting trial.
Most personality disorders are first diagnosed in adolescence or in early childhood where they are often labeled “conduct disorders,” including the milder variant seen in younger children called “oppositional defiant disorder.” Conduct disorders are “the most common reason for referral to child and adolescent mental health services in Western countries” and are becoming more frequent.
“Untreatable” has always been a defining characteristic of personality disorders, because symptoms reflect ingrained patterns of thinking and behavior. Also, because of difficulty thinking clearly, many sufferers lack insight or awareness about their condition, called “anosognosia” from the Greek meaning to not know a disease.
Most sufferers have such trouble getting along with other people that they rarely seek treatment and, when they do, often drop out. Patients with BPD, the most commonly treated personality disorder, quit treatment programs about 70% of the time, according to “Treatment for the ‘Untreatable’” in the American Psychological Association’s Monitor.
Newer methods have had better success based on a combination of group and individual treatment, such as Dialectical Behavioral Therapy (a skills-based approach teaching management of emotions and improving relationships) and Schema-focused therapy (identifying unmet needs that have led to negative life patterns).
As “Killing Eve” continues, the psychopath label seems less apt for Villanelle, because she is a hired hit woman. She kills those she is asked to kill, whereas “when female psychopaths kill, the motive is usually money, or attention, and the victims are people they know.” (When male psychopaths kill, usually the motive is psychosexual and the victims are strangers.) Also, Villanelle is at times “genuinely thoughtful…and charming.”
—Mary Carpenter
Every Tuesday in this space, well-being editor Mary Carpenter reports on health news you can use.
NEARLY IDENTICAL bumps on two adjacent fingers—which I was hoping the dermatologist could remove—were not the same thing, the P.A. told me. One was a cyst, for which I would need a hand specialist. The other was a wart, which she advised working on myself to remove with salicylic acid patches, despite my entreaties for the cryosurgery that had so rapidly removed my kids’ warts years ago.
Cysts and warts can appear similar and both come in dozens of varieties that are grouped based on appearance and location. Both often resolve with no intervention. Both carry a small risk of cancer: warts, when the virus causing them is one of the few high-risk strains; and cysts, if the cells inside them are cancerous.
Cysts are abnormal capsules or sacs that occur within tissue and are usually closed and separated from nearby tissue by a distinct membrane. A cyst fills with liquid or gaseous material— like a blister—or pus, which makes it an abscess.
Cysts can vary in size from microscopic to large enough to displace internal organs, in which case doctors can remove them surgically. Most “live in” in the skin, ovaries, breasts or kidneys.
Two kinds of cysts occur beneath the skin. A sebaceous cyst is filled with the oily substance called sebum, secreted to lubricate the skin—which can build up inside a pore or hair follicle. An epidermoid is created when surface skin cells move deeper into the skin and fill with soft, yellowish keratin. (When I had a sebaceous cyst that occasionally became red and enlarged, I asked the dermatologist to remove it before a long trip to southern Africa where I wanted no extra health risks.)
Ovarian cysts are most often benign, although some grow large enough to make a woman appear pregnant. While ovarian cysts are less common before menopause, up to 18% of women will have one at some point, and a small percent of these will become cancerous.
Baker’s cysts create a bulge and feeling of tightness behind the knee, most often causing pain when extending the knee or during exercise. They’re usually caused by joint problems like arthritis. Pilar cysts form from hair follicles, most commonly in the scalp. When cysts arise due to a chronic medical condition, like fibrocystic breast disease or polycystic ovary syndrome, that condition becomes the focus of treatment.
Warts, by contrast, are small tumors on top of the skin caused by the human papilloma virus (HPV). Ranging from very light colored to very dark, they are usually painless but can cause burning and itching. Different types include common warts, usually on the fingers; plantar warts on the soles of feet; flat warts that occur where you shave; and genital warts.
HPV triggers the growth of extra cells that develop their own blood supply and nerves. The virus is contagious—passed when skin is shed directly onto another person or onto a floor or carpet. Although warts can spread through sexual contact, most are passed via casual contact or shared objects like towels. Untreated warts can last about two years until the skin recognizes the virus and begins fighting back.
The HPV vaccine Gardasil—usually given to people ages 9 to 26—prevents many kinds of warts and, importantly, prevents most cancer that can be caused by some strains of HPV. In adults, warts are worrisome only when they appear suddenly, possibly signaling immune system malfunctioning; otherwise, by adulthood, most people have developed immunity to the virus.
To remove warts, dermatologists usually recommend salicylic acid, but a reportedly easier and more effective remedy involves duct tape. You cover the bump for six days, and then on the seventh day remove the tape, soak, and remove dead skin with an emery board. Other options include lasers, freezing and surgery.
For my cyst, an orthopedic hand specialist recommended aspirating the fluid with a needle, which was unexpectedly painful. In the months afterwards, the cyst became infected and required surgical removal, for which I waited a little too long and lost some function in the adjoining tendon.
At a subsequent dermatology visit for a whole-body exam, after months of using salicylic acid on the wart to no avail, I asked again about cryosurgery. But when the P.A. gave that bump a second look, she switched the diagnosis: It’s a cyst and needs a repeat visit to the hand doctor. Now I’m waiting for real trouble before starting down that road again.
—Mary Carpenter
Every Tuesday in this space, well-being editor Mary Carpenter reports on health news you can use.
AFTER TRAVELING to Africa every few year for decades, filmmmaker K.R.R. had to add the measles vaccine to her medical to-do list for this summer’s visit. That’s because of the recent global surge in measles cases and because she was born in 1957 (considered the cut-off year for having acquired immunity).
In the U.S., people are asking these questions: how dangerous is the disease, and who needs the vaccine? The numbers of measles cases here continue to climb with every passing week—from more than 700 during April to more than 800 so far for May—but still much lower than the more than 17,000 cases in the outbreak of 1989.
For those born before 1957, the risk of contracting measles—and any serious risks—are very low due to immunity from frequent outbreaks that occurred during the 1950s. Those born during or after 1957 who cannot document having had measles or being vaccinated with live (vs. killed) virus should receive at least one dose of the vaccine.
But CDC Vaccine Director Nancy Messonnier recommends that all adults who travel internationally, those living in communities with ongoing outbreaks and those spending time in high-risk settings like hospitals check their status to make sure they’re protected.
The possibility of measles causing serious illness after early childhood is also very low. But for infants and children younger than five years old who get measles, almost one-third require hospital treatment. Hearing loss occurs in about one in ten due to ear infections, and one in 1,000 due to encephalitis (swelling of the brain).
About one of every 20 children who get measles will contract pneumonia, the most common cause of death. Between 1987 and 2000, for every 1,000 reported cases, two to three died from pneumonia and there was one case of encephalitis, which can also cause convulsions and intellectual disabilities.
The current outbreak has been traced to the rising numbers of unvaccinated children and the resulting decrease in herd immunity —”that cushion of immunity that helps all of us,” explains Messonnier.
Because a few people in every population—usually due to poor health—cannot receive vaccinations, the percentage that needs to be vaccinated to protect the entire population is based on each disease’s ease of transmission. For highly contagious measles, that number is around 95%, compared to 80-85% for polio.
The measles virus spreads via droplets that remain alive in the air for up to two hours after an infected person coughs or sneezes. Symptoms don’t show up until 10 to 14 days after exposure, and a person is contagious for four days both before and after the rash appears.
The outbreaks have been concentrated in four states: New York, New Jersey, Washington and California. Of those, the majority of cases (at a recent count, almost 500 out of little more than 700) have occurred in Orthodox Jewish communities in New York City and Rockland County, north of Manhattan, mostly because of parents who choose not to vaccinate their children. Locally, for 2019, Maryland has counted five cases; and DC and Virginia, none.
But responsibility also goes to the global surge in measles cases. These are up more than 300% in the first quarter of 2019 compared to the same period in 2018—a rise that the WHO considers “alarming” and “a global crisis”—with flare-ups occurring in France, Greece, Israel and India.
“When we see large measles outbreaks in countries that are common destinations for U.S. travelers like we’re seeing this year,” says CDC senior measles analyst James Goodson, “that’s when we often see the largest number of measles cases in the U.S.”
For adults, the main reason to get checked or vaccinated for measles is not to infect very young children or grandchildren. Measles is on the list of top five vaccines to get if you’re around young children. The others are influenza; pertussis, or whooping cough (Tdap vaccine includes a tetanus booster); pneumococcus (against the bacteria that cause pneumonia); and shingles (to prevent risk of spreading chickenpox, caused by the same virus as shingles.)
—Mary Carpenter
Every Tuesday in this space, well-being editor Mary Carpenter reports on health news you can use.
ANECDOTAL ACCOUNTS of health benefits of CBD (a non-psychoactive ingredient of the Cannabis plant) are pouring in from the medical establishment and personal experiences, while research allocations and sales numbers are soaring.
Between 2014 and 2018, the NIH budget for CBD studies went from zero to about $16 million; and CBD sales rose from $100 to $500 million and are projected to exceed $20 million by 2022. Last year, the first CBD product received FDA approval for treating two kinds of epilepsy.
But last month, FDA commissioner Scott Gottlieb warned consumers about the unsubstantiated health benefits of CBD: “These products have not been shown to be safe or effective…deceptive marketing of unproven treatments may keep some patients from accessing appropriate, recognized therapies.”
“The science just isn’t there yet,” Columbia University neurobiologist Margaret Haney told ScienceNews. In Haney’s view, “a gaping chasm separates the surging CBD market and the scientific evidence backing it,” and “messages of CBD’s purported health benefits come from people trying to sell CBD products—not from scientists.”
What Forbes calls the “CBD explosion” took off when industrial hemp—a variety of the Cannabis plant—became legal under the 2018 Farm Bill as long as it contained less than .3% [psychoactive] THC.
But the distinction between the two Cannabis varieties has been changing. Previously, industrial hemp—grown for fiber and seed oil —was a very different plant from the “drug” plant, explains marijuana historian Martin Lee. The key difference used to be the quantity of resin (the source of cannabinoids such as THC and CBD), which are both abundant in marijuana plants but were both almost non-existent in hemp. Also, because of the extraction process, CBD from hemp was more likely to be contaminated by pesticides and heavy metals in the soil.
“The distinction between hemp and other forms of cannabis is fast becoming moot,” according to Lee—notably in the quantities of CBD and THC they contain, although hemp remains legal where marijuana is not. As long as THC levels remain below .3%, high-resin cannabis varietals can qualify as hemp—even when CBD levels approach double digits.
CBD products from hemp are preferred by those who fear the possibility of psychoactive effects —euphoria, sedation—from whatever THC might be present in marijuana-derived CBD. On the other hand, people taking CBD at higher doses report side effects that include fatigue, along with nausea and irritability.
Dosage listed on labels of hemp-derived CBD, which is classified as a supplement and thus unregulated, can be unreliable. In a 2017 study of CBD products, 43% contained less CBD than labeled, while 26% contained more. And in previous FDA testing, some samples contained none.
Cannabinoids extracted from the marijuana plant, on the other hand, are classified as medicine and subject to oversight by the FDA and state regulators. So, for example, marijuana-derived CBD products can be sold in Massachusetts dispensaries that are prohibited by law from providing CBD extracted from hemp.
Most CBD research showing positive medical effects involves preparations from the marijuana plant that contain some THC—as well as high doses of CBD—legally available only to people with medical marijuana cards in 33 states and DC, and often costly. In states like Colorado that allow both medical and recreational marijuana, dispensaries can sell the same products to all consumers, with or without cards.
“Anything we know about CBD for pain comes from research where…you’re looking at the combination of THC and CBD and various components of the plant,” according to Temple University researcher Sara Jane Ward, who has studied CBD over the past twelve years.
And in one study, the 15 men who took 300 mg of CBD became calmer during a stressful public speaking task, compared to those receiving a lower or higher dose (commercially available CBD doses usually hover around 10-20 mg).
On the other hand, doses as low as 25 mg/d decreased anxiety scores for almost 80% of patients, while sleep scores improved for 66% but fluctuated over time, according to a report by psychiatrist Scott Shannon at the University of Colorado, Denver.
“CBD may prove to be an option for managing anxiety, insomnia and chronic pain,” writes Boston clinician and Harvard professor Peter Grinspoon. CBD can alleviate and even eliminate discomfort, but neither CBD nor THC help with severe pain. But adding THC “does increase the analgesic effect of CBD,” according to Grinspoon’s Harvard Health blog.
Walnut Creek, California, clinician Rachna Patel agrees, observing good results with CBD for mild to moderate levels of pain, but that these are “less likely” for severe pain; and for shingles and spinal pain, “some amount of THC is needed.”
Among patients at a Portland, Oregon, pain clinic who report taking CBD, about half say they get some benefit and about half say they didn’t notice anything, according to pain clinician Kimberly Mauer.
Topical CBD has helped control skin diseases such as eczema, psoriasis and acne via anti-inflammatory effects and regulation of immune system imbalances. But, according to Denver dermatologist Robert Dellavalle, “The most promising role for cannabinoids is in the treatment of itch.”
The best advice for CBD consumers is to choose products labeled with clear information about dosage and ingredients. A COA or Certificate of Analysis should include any added ingredients like corn syrup as well as testing done for heavy metals and pesticides. “Broad spectrum CBD” contains all of the plant’s naturally occurring compounds except for THC, while “full spectrum” includes THC, and “CBD isolate” is the compound in its purest form.
Additional ingredients can include “complimentary cannabinoids, terpenes and plant-based adaptogens,” writes Sherrie Nachman on Forbes. Nachman believes the inclusion of these ingredients can be more important than dose in determining the effectiveness of a product.
CBD—either ingested or absorbed through the skin—interacts with the body’s natural cannabinoid receptors “in areas where we’re most deficient—which is why CBD is also considered an adaptogen,” according to Nachman. And that’s the reason CBD affects individuals so differently, based on the different amounts of natural cannabinoids each person’s body is already producing.
Forbes writer Terrell Davis suggests keeping a CBD journal to record which products you try, their level of CBD and how that CBD affects you—and to experiment with different amounts of CBD as well as with other cannabinoids to figure out what works the best.
Meanwhile, marijuana regulations, both federal and state, continue to hamper CBD researchers by making it hard to acquire adequate material for their studies. University of Colorado, Boulder, neuroscientist Kent Hutchison and others have created a mobile pharmacology lab called the CannaVan to collect data on people who’ve taken products they’ve purchased on their own—currently focusing on the CBD’s effects on anxiety and pain.
When Florida clothes designer L.K. tried two different strengths of CBD-only preparations, she found “the weaker one seems to do nothing, and the stronger strength makes me feel woozy.” A third preparation with a little THC (8:1) “seemed to take an edge off my anxiety…perhaps not enough as I am back on Paxil.”
Using my D.C. medical marijuana card, I have received several preparations for chronic pain (including both THC and CBD), but each one put me to sleep too quickly to judge any other effects. I let my card lapse but remain hopeful that the booming interest in marijuana-based preparations means better possibilities coming down the pipeline sometime soon.
—Mary Carpenter
Every Tuesday in this space, well-being editor Mary Carpenter reports on health news you can use.