WRITING DOWN answers to Cognitive Behavior Therapy (CBT) questions— in a small CBT workbook handmade by a friend—led me to a startling revelation: Self-directed CBT that requires written responses works better for me than previous efforts employing “self-talk,” which ranged from how-great-I-am mantras to reframing negative thoughts, a la Brené Brown.
(What my friend said inspired her gift was that she herself had found the exercises helpful. But I suspect that a bigger reason may have been that listening to me get upset about the same family issues over and over made her think I might benefit—and even not need to talk about them so much … .)
As surprisingly impressed as I once had been after watching therapists’ video recordings of CBT sessions—at how these sessions provided dramatic help to patients—I have been more so by the power of my friend’s gift. One advantage for me may be the book’s unintimidating 7-inch-by-5-inch size; full-size, commercially published CBT workbooks, notably Retrain Your Brain: Cognitive Behavioral Therapy in 7 Weeks by University of Pennsylvania psychologist Seth Gillihan, abound.
“One of the goals of CBT is to become your own therapist by learning skills you can use on your own,” writes Gillihan in a National Alliance on Mental Illness (NAMI) blog, adding: “What drew me to CBT was how straightforward and intuitive it was, which also makes it well-suited for self-directed therapy.” In addition, Gillihan describes two reviews, each including more than 30 studies, that found “self-help treatment significantly reduced both anxiety and depression, especially when the treatments used CBT techniques.” “The central idea behind CBT is extremely simple: If you change the way you think, you can change the way you feel,” writes nurse and blogger Risa Kerslake. “But if feeling better…were that easy…” Kerslake describes her “anxiety hangovers,” waking up on the day after an event feeling horrible about everything.
Using the “triple column technique” for written, self-directed CBT, Kerslake explains that “negative self-talk, that crappy mean little voice inside your head,” goes in the first column. In the second, she records cognitive distortions—described by Cleveland Clinic as “unhelpful patterns of thinking…based on problematic core beliefs, including central ideas about yourself and the world.”
Distortions, such as “‘should’ statements,” “personalization (self-blaming), “overgeneralization” and “jumping to conclusions,” arise in statements “the little voice makes about who I am and what’s going on in my life,” writes Kerslake. By writing down these little-voice statements, she notes, “it always looks kind of shocking to see [them] in print.” Writing down upsetting thoughts can make it easier to view them with distance and more logical thinking, to see the “cognitive distortions,” and then to respond to the subsequent questions and ultimately come around to a less fraught way of thinking about the experience. (The little book from my friend includes “20 Cognitive Distortions,” along with short descriptions for each.)
The “Wheel of Emotions” on another page of my book depicts colorful rings that expand outwards and contain words describing feelings. The wheel is “especially useful for moments of intense feeling and when the mind cannot remain objective as it operates from an impulsive ‘fight or flight’ response,” writes Hokuma Karimova on Positive Psychology. The goal is not to replace negative motions with positive ones but to identify and accept an emotional experience.
The wheel’s central circle lists primary or basic emotions—such as scared, sad, mad and glad—with different iterations of the wheel employing variations in the number of emotions and their labels. Moving outwards, subsequent rings include different combinations and intensities of emotions so that anger can mean anything from annoyance to fury while fear ranges from timidity to terror.
“This Wheel of Emotions diagram beautifully depicts the relationships between each emotion in the form of a spectrum,” according to Therapist Aid. “We like to use this worksheet with clients who have a hard time picking out the right word to describe how they feel. Even if the word they want isn’t on the spectrum, they might be able to point out what it’s near.”
My book’s final section encourages writing with tear-off workbook pages that pose five questions and leave blank spaces for recording answers. The first three questions ask for descriptions of “What happened?” “What is going through your mind?” and “What emotions are you feeling?” The final two encourage reflection: “What thought patterns do you recognize?” and “How can you think about the situation differently?”
For me, the main reason I actually performed self-directed CBT may be the kindness of my friend who put together my little book with paper, glue, cardboard, ribbon and a cover of decorative paper. Also the small size of the book and the spaces for writing made the work appear relatively undaunting. While I tried the three-column method only once, I have continued to use the little book.
“What happened” to me recently, for example, was running into R.L., a long-time friend who greeted me with a smile and cheery “hello,” despite having dropped me about five years ago with no explanation. “What was going through my mind”: I must be deeply flawed or have done something unforgivable to cause her to drop me. For “emotions,” I wrote: victimized, powerless, vulnerable, abandoned, which fall into the wheel’s “Sad” section; along with some from the “Anger” section, including irritated and embarrassed.
The first cognitive distortion I listed was “self-blaming, which led me to emotions such as inadequate, worthless, insecure–listed in the “Fear” section of the wheel. For “Challenge Your Thoughts,” I remembered that R.L. had dropped at least one very old friend during the period of my friendship with her. Also, I noted that I had made wonderful, loyal friends over many decades. After writing, I breathed a little more easily; also I hoped never to give R.L. another thought.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
AT HER annual physical exam, C.W.’s internist suggested she think about the “cancer blood test” called Galleri —even handing her a leaflet to take home. What interests physicians in the handful of multicancer early detection (MCED) tests is the possibility of finding more than 50 types of cancer—early enough to treat and even cure; and, in Galleri specifically, that the British national health system is now conducting a huge research study to determine which people might benefit.
“Because the English system is known for cost-consciousness, we are paying attention,” said DC internist S.P. Most U.S. insurers, including Medicare, do not currently cover the $1,000 to $1,600 cost of the Galleri test. Among questions the NHS-Galleri trial hopes to answer, according to Healthline , is “one of the big unknowns …whether or not using it as part of cancer screening will help to improve people’s outcomes and save lives.”
The best target population, with the so-called “highest yield”— referring to age- and risk-groups —is another important question. Also as noted in news articles, the Galleri leaflet refers to “adults with an elevated risk for cancer, such as those aged 50 or older.” Ultimately, figuring out the target population depends on identifying not just which cancers the tests detect, but those for whom early detection can result in a cure.
“Someday this [blood testing for cancer] will become routine for people who are at high risk. But we’re not there yet,” Director of Scripps Research Translational Institute Eric Topol told Bloomberg. Also, the best cancer blood testing may ultimately involve a combination of existing MCED tests, which, Topol said, “have taken pretty drastically different approaches.” MCED tests “may not work as well as a colonoscopy or mammogram,” American Cancer Society’s Chief Scientific Officer William Dahut told Bloomberg. Looking for some of the most common cancers, these traditional tests can also locate pre-cancerous cells in polyps or lumps, which can be removed during the test or soon afterwards to reduce the risk of cancer.
The expectation for MCED tests, however, is that they will supplement traditional assessments because they can pick up signs of less common cancers for which doctors don’t usually screen or with symptoms that are harder to diagnose. With ovarian cancer, for example, a doctor performing a pelvic exam cannot easily feel a small tumor because of its location within the body. Also difficult to detect are more than 70 soft-tissue sarcomas, which form in tissues that connect, support and surround other structures and can include muscle, fat and nerves.
MCED testing’s main advantage is the ease of adding it to a routine doctor’s office visit. But a major concern is the possibility of unreliable results. False-negative results would create a false sense of security if the test failed to detect cancer—either because the MCED testing is unable to detect all types of cancer or because it can be inaccurate in detecting cancer-related signals.
False-positive results, which would incorrectly indicate that cancer is present, are another risk, because these could cause unnecessary anxiety and lead to additional testing. A 2021 British “validation” study, however, assessed the Galleri test’s accuracy in 2,823 people with a known cancer diagnosis compared to 1,254 healthy people. The study found 99.5% specificity, or accuracy, in determining when a person had no cancer-related signals, making the risk of false-positives impressively low.
Importantly, the Galleri test correctly identified the cancer’s origin site in 88.7% of study participants already diagnosed with cancer—a determination that can take a week or more using current methods, which can sometimes fatally delay the beginning of treatment. With an overall sensitivity in correctly detecting cancer at 51.5%, the test’s sensitivity increased as cancers became more advanced.
Given to asymptomatic adults at higher risk for cancer, MCED tests look for proteins or genetic factors, for example in “cell-free” or circulating DNA that has been released from cells—which reveal patterns of changes that indicate the presence of cancer as well as where the cancer started.
Traditional blood tests that can reveal signs of cancer include the complete blood count (CBC) that measures types of blood cells (platelets, red blood cells and white blood cells), but are mainly useful for “blood cancers,” such as leukemia and some lymphomas. And different blood tests, usually performed only when symptoms suggest cancer, look for “tumor markers” that are produced either by cancerous cells or by the body’s normal cells in response to cancer; or for proteins, immunoglobulins released by the immune system in response to specific cancers.
For me, the possibility of finding cancer early enough to cure makes MCED testing hard to resist. But I am hesitant because of the high price tag and because the results provide only a single snapshot in time: the possibility that new cancer cells could begin growing the next day suggests the need for repeat testing on a regular basis. As a result, I will wait for insurance coverage, expected in the next year or so based on results from the British study. Recently attempting to schedule a colonoscopy, on the other hand, I found that the first appointment was not available for five months.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
A response to a reader’s question: Is malaria spreading in the U.S.?
RECENT REPORTS of seven malaria cases in the U.S. sound like a small number—but what’s important is the description “locally acquired,” meaning that local mosquitos in Texas and Florida are carrying a parasite that had not been seen in the U.S. since 2003. In addition, the cases diagnosed in the past two months appear unrelated to each other.
Anopheles mosquito vectors found “throughout many regions of the country are capable of transmitting malaria if they feed on a malaria-infected person,” according to the CDC’s recent “Health Advisory” that warns in bold print: “Malaria is a medical emergency.” The advisory directs clinicians to “consider a malaria diagnosis in any person with a fever of unknown origin”—specifically noting “regardless of their travel history.”
More likely in the Northeast, however, the West Nile virus is “the most important mosquito-borne disease in North America,” according to Connecticut Agricultural Experiment Station mosquito expert Dr. Theodore Andreadis. Most people infected with West Nile have either no symptoms or mild flu-like fatigue and aching, but risk of severe disease increases with age: each year in the U.S. more than 1,000 people develop inflammation of nervous system tissues that can lead to encephalitis or meningitis.
Washington DC ranks number four on the 2022 Top Mosquito Cities list kept by Orkin, the pest control company. The highest numbers of West Nile cases occur in major urban areas —Los Angeles, Chicago and Dallas-Fort Worth — although the Great Plains states (North and South Dakota, Wyoming and Colorado) have the highest rates. According to Climate.gov, the “largest identified single outbreak” in U.S. history occurred in Arizona in the summer of 2021 — traced to a “wetter-than average monsoonal season.”
Two other mosquito-borne viruses —reported, though rare, in the Northeast —with names that reflect their symptoms of severe joint and muscle pain: Dengue fever, with the nickname “breakbone fever;” and chikungunya, from an African word meaning “to be contorted,” according to the Washington Post. The Aedes mosquitos carrying these viruses “love living around humans” and —though more prevalent in U.S. territories, notably in Puerto Rica, and elsewhere in the world —have made recent gains in Southern California, “infuriating the region’s residents.”
(The deadliest but very rare mosquito-borne virus in the U.S. is Eastern equine encephalitis (EEE), which occurs mostly in rural areas close to freshwater swamps. The virus causes death in about 30% of cases, and permanent neurological damage in around 70% of those who survive the infection.)
The Asian tiger mosquito (ATM), however, “can become the single most important pest species once it gets established,” according to Amdro pest services. Another species of Aedes, the ATM —with its distinctive white stripes, including one down the middle of the back on a black body—is a silent, aggressive human biter that bites during the daytime. The resulting flattish, blister-like spot can have a red halo that spreads outwards, and it feels hot, itchy and painful. For some people, both the itching sensation that usually subsides rapidly can reactivate with changes in temperature, such as after a hot shower, and the intense pain can persist for several days.
In the eastern U.S., Asian tiger mosquitos are carrying West Nile virus but have not yet caused proven disease. More worrisome, they are potential vectors for other arboviruses—viruses caused by mosquitos and ticks—including EEE, chikungunya and Zika. The expanding range of Aedes may be the result of climate change, related to changes in temperature and precipitation.
Malaria, however, could be the most worrisome mosquito-borne disease in the U.S.: Without early diagnosis and treatment, it can progress to severe disease or death. Symptoms include chills, headache, myalgias and fatigue that can begin anywhere from 10 days to four weeks after infection. Every year in the U.S., of some 2,000 cases of “mostly travel-related malaria,” about 300 people develop severe disease, and five to ten die. (Malaria can also be transmitted from mother to fetus or neonate and through blood transfusion and unsafe needle-sharing practices.)
For mosquito-borne disease, the main advice is to seek treatment for unexplained or enduring symptoms, especially fever. Otherwise, make efforts to avoid mosquito bites that include wearing light-colored, loose clothing and using mosquito repellent —to protect against all mosquito species, these would be necessary day and night.
Regardless of protective measures, some people are more likely than others to attract biting mosquitoes—notably those with Type O blood, who seem particularly enticing to the Asian tiger mosquito. And mosquitoes seem to like body heat as well as sweat, because it contains lactic acid and ammonia—raising the risk of bites following exercise; and carbon dioxide, which increases with greater exhales—both during exercise and for larger people.
Also, mosquitoes appear drawn to people who have eaten sweet, salty or spicy foods, as well as those high in potassium, notably bananas. And the bugs gravitate toward people in green and black clothing, rather than those wearing white and gray—maybe because darker colors are easier for them to see. Finally, mosquitoes may head for forearms, ankles and feet, likely because the skin in these areas can have higher levels of bacterial growth.
A female mosquito’s bite —labeled a “blood meal” because the blood provides nutrients the mosquito needs —leaves behind saliva that can spread a multitude of infections. The Washington Post calls the mosquito “the deadliest animal in the world…smaller than a pencil eraser and weighs around two-thousandths of a gram — less than the weight of a single raindrop.”
—Mary Carpenter regularly reports on topical subjects in health and medicine.
Editor’s Note: While updating her 2017 post on Blue Zones, Mary Carpenter found healthy lessons from the world’s original five Blue Zone regions—those with the world’s highest percentages of centenarians—spreading to communities around the U.S. Although critics note weaknesses and inaccuracies in the data, most everyone applauds healthy Blue Zone practices, such as eating less food and moving more often.
“THE RESULTS are stunning,” proclaimed Harvard nutrition researcher Walter Willett, referring to “double-digit drops in obesity, smoking and BMI,” reported by the Blue Zones Project organization. What can work better than individuals struggling to make healthy changes is the supportive social structure offered by Blue Zones communities—along with specific policy and environmental changes, such as building sidewalks and paths to create a more walkable environment.
“We aren’t competing with one another, we’re helping each other be successful,” one community participant told Oprah. “It helps to have everyone around you thinking and acting healthier.” The success of Blue Zones programs may come from an “easygoing approach” that urges participants to make small changes–for example, commit to weekly walks at work—rather than to follow challenging exercise routines or restrictive eating rules.
“Putting the responsibility of curating a healthy environment on an individual does not work,” according to author Dan Buettner, who worked with a team from National Geographic to identify the world’s first five Blue Zones—regions in Greece, Sardinia and Costa Rica, along with Okinawa, Japan and Loma Linda, California. The Blue Zones Project—now in “hundreds” of U.S. communities, from beach towns in Florida and California to some 15 towns across Iowa—focuses on the so-called “Power 9” lifestyle changes, with many catchy labels.
“Right tribe,” for example, refers to living in social circles that support healthy behaviors. And “Plant slant” refers to the Blue Zone longevity diet “cornerstone” of beans (including fava, black, soy and lentils) as well as consumption of little meat, on average five times a month and in small portions.
An alternative to Blue Zone community life, vacations on Costa Rica’s Nicoya Peninsula—one of the original Blue Zones—offer the local “big secret,” according to Buettner: “the three sisters of Mesoamerican agriculture, beans, corn and squash.” Located on the northwest coast of Costa Rica around the surfing town of Nosara, lodgings range from boutique hotels and bungalows to an Airbnb treehouse, and offer healthy amenities, such as yoga and spa treatments.
Critics note, however, that longevity data from the original five Blue Zones may be inaccurate. According to a BBC report, of more than 200,000 Japanese reportedly older than 100 years of age, many were missing or dead and only about 40,000 could be located at fixed addresses. Oxford University sociologist Saul Justin Newman points to high rates of smoking and alcohol consumption along with low average lifespans in some Blue Zones.
The greater the number of supercentenarians, the lower the life expectancy in these impoverished, unhealthy communities, according to Newman, which may be due to faulty record-keeping or to pension fraud: people misreporting their ages to collect illegal pension payments. Writes Harriet Hall on Science-based medicine, Blue zones may be a myth; also, Okinawan longevity “may be a thing of the past.”
Okinawa is the Blue Zone reporting the greatest number of centenarians along with the lowest median lifespan. According to Newman, the region has the worst over-65 dependency ratio; ranks first in the nation for obesity and last for consumption per capita for fruits and vegetables; and “has some of the highest levels of clinical depression in Japan.”
But Okinawa is also the source for three of the Blue Zones Project’s Power 9 pillars: “Right Tribe,” from Okinawan moais, groups of five friends committed to each other for life; “Purpose,” from ikiga, explained as “why I wake up in the morning; and the “80% Rule,” from the hara hachi bu mantra Okinawans repeat before meals to remind themselves to stop eating when their stomachs are 80% full.
Of the remaining pillars, “Move naturally” advises living in environments that promote “constant moderate physical activity,” such as gardening, rather than intense exercise routines; “Downshift” suggests daily de-stressing, for example, with a nap or happy hour; and “Belong” refers to joining a faith-based community. Finally, “Loved ones first” involves care for aging relatives and commitment to a life partner: putting family ahead of other concerns is the No. 1 variable on the Venn diagram of overlapping Blue Zone longevity measures.
The Vitality Compass, developed by Buettner along with the University of Minnesota School of Public Health—named Best Online Tool for Retirement and Longevity by the WSJ—includes questionnaires based on the Power 9 and provides users with “12 customized recommendations to help them live longer and better.” Taken as an initial baseline and then again three to six months later, the Compass can be helpful for assessing progress.
In six years beginning in 2009, the three Southern California beach towns working with the Blue Zones Project reported the number of overweight people dropping nine points to 50.8 percent—while the national rate rose four points to 63.7 percent. After the creation of Blue Zone communities in Iowa, the state’s healthiest states ranking improved from #16 in 2011 to #10 in 2013.
The Blue Zones website has 10 food recommendations with additional catchy labels, starting with the “95/5 Rule: Eat plants” – advising that 90-95 percent of your food should be fruits, vegetables, grains, greens and beans. Others are “Retreat from Meat,” “Take or Leave Fish” (because “modern-day fish has become so contaminated with pesticides and other chemicals”) and “Diminish Dairy” (with an egg limit of three per week).
But a Blue Zone diet may not exist, according to Hall and others—who point to the almost identical precepts found in the universally recommended Mediterranean diet, as well as to vast differences in eating preferences among the original Blue Zones. The Ikarians’ diet is notable for “its emphasis on potatoes, goat’s milk, honey, legumes, wild greens, some fruit,” according to Buettner. The longest-lived Sardinians also consume large quantities of goat’s milk, as well as sheep’s cheese—including a sharp pecorino, with high levels of healthy omega-3s —along with bread, fennel, tomatoes, almonds and wine. And Seventh-Day Adventists in Loma Linda follow a “biblical” diet focused on grains, fruits, nuts and vegetables; and they drink only water.
While trying to follow general Blue Zone precepts, I have trouble with the specifics —determining when my stomach is 80% full; or, the suggestion to “Move naturally,” forgoing “mechanical conveniences for house and yard work.” I am not involved in a faith-based community, and digestive issues prevent me from eating many beans. Mostly I worry that residence in a Blue Zone community would heighten already-existing pressures to improve my diet—notably by reducing salt and sugar—along with disapproval of regular lapses that include ice cream and cookies.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
“MY OXYGEN level is 93 [compared to] 98 and 99 before Covid . . . my doctor says my inflammation is rampant and my antibodies for Covid are enough for an elephant,” said Florida watersports enthusiast C.T., in his early 70s, who remains too fatigued to enjoy his daily pre-Covid kite-sailing, paddleboarding and windsurfing. “The thing that jumped out at me was the Epstein-Barr being triggered . . . went from 18 to 600 and 800 over the last year that I’ve had Long Covid.”
Alarming numbers aside, what’s most debilitating for C.T. is post-exertion malaise (PEM), the so-called “energy crash” that can follow physical exertion, often worsens over time and creates a life-changing burden for hundreds of thousands of Long Covid sufferers. According to Nature, PEM “fatigue is a subjectively perceived exhaustion that follows disproportionately after exertion and does not improve adequately after sleep or rest” — and is the most frequently reported symptom among post-Covid syndrome (PCS) patients.
Many physicians who struggle to help PEM sufferers are now voicing their excitement about possible treatments emerging from extensive research on Long Covid. In addition, the treatments might help an enormous number of people suffering from a variety of other conditions—notably myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), believed also to be a post-viral condition, which shares PEM symptoms with Long Covid.
For the first time, PEM has a single cause—the Covid virus—which provides an enormous boon for researchers. In contrast, for previous research on ME/CFS, assessing symptoms proved challenging, and diagnosis often came years after extensive damage to the body had already occurred.
“The contribution of Long Covid is an N [number of patients] so big—all having the same, well-documented original infection,” said one local D.C. internist. An estimated 23 million people, about 10% of those infected by the Covid virus, report symptoms lasting seven months or longer, according to initial findings from the Research Covid to Enhance Recovery (RECOVER) trial. Of 12 symptoms highlighted by RECOVER, number one is PEM—reported by around 70%—with dyspnea (difficulty breathing), by around 55%.
The RECOVER trial, begun in October 2021, has to date enrolled more than 8,500 adults—from an original database of more than 7 million people who had been sick with Covid and reported symptoms lasting more than three months. Trial participants continue receiving whatever treatment they or their doctor has chosen and undergo different tests or measurements depending on their personal health.
Recently, however, research on PEM has led patients and patient advocates to protest against RECOVER testing that involves increasingly intense physical challenges—concerned that participants will not be well informed about potential risks, and that researchers will not sufficiently monitor people for harm after the exercise regimen or after the trial concludes. ME/CSF patients with PEM have reported that “continuously pushing past their limits has caused [their symptoms] to permanently worsen.”
“I now think of Covid as a neurological disease as much . . . as a pulmonary disease,” said UCLA physician William Pittman. “And that’s definitely true in Long Covid.” Cognitive difficulties for Long Covid patients include difficulty with memory, attention, sleep and mood; and PEM also involves nerve dysfunction, often in the autonomic nervous system — called dysautonomia.
“Persistent viral loads or remnants hidden away in the tissues and causing chronic inflammation” may explain Long Covid symptoms, according to Yale researchers. Other theories point to inflammation in the brain due to increased auto-immune activity—which lasts beyond the acute Covid infection, or which is stimulated by the reactivation of dormant viruses such as Epstein-Barr.
PET scans have detected evidence of brain inflammation in patients with Long Covid, according to Canadian research published in late May from the Campbell Family Mental Health Research Institute. Said Neuroimaging Program Head Jeffrey Meyer, “We already knew that there is brain inflammation in people who died in the midst of a severe, active COVID-19 infection. What’s new about this study is that it shows that inflammation is hanging around for a long time in the brains of people with long COVID even after only mild to moderate symptoms of active COVID-19.”
The possibility that Long Covid symptoms are caused by lingering viral remnants offers hope that it might be necessary to extend treatment with antiviral drugs such as Paxlovid beyond the current regimen of five days to completely clear the Covid virus from the body. And if one cause of Long Covid is a chronic autoimmune response, anti-inflammatory drugs, such as metformin, could help treat the symptoms. In a multi-center study, 564 overweight or obese adults who started a two-week course of metformin while suffering from acute Covid had a 42% lower chance of being diagnosed with Long Covid compared to those who took a placebo when they first got sick.
Yale Medicine is now recruiting participants for a new study, Listen to Immune, Symptom and Treatments Experiences Now (LISTEN) that will investigate Long Covid along with other pathogens causing chronic illness in a “subset of people, called post-acute infection syndrome (PAIS), which includes ME/CFS” — another example of how the research spurred by huge numbers of Long Covid patients could help sufferers of other PAIS, such as that following Lyme disease.
For my symptoms that lingered following acute Lyme infection, notably peripheral neuropathy, my internist prescribed several additional weeks of doxycycline treatment – under the same theory as that for Long Covid, that ongoing issues might be occurring as the result of infectious remnants, in my case of the bacteria causing Lyme disease. While the effort did not help me — and the final verdict is not in on adding more days of Paxlovid — my only issue is wobbly walking, nothing like the disabling fatigue suffered by C.T. with PEM.
—Mary Carpenter regularly reports on topical issues in health and medicine.
If this post was sent to you by a friend, you can sign up for the newsletter at the very, very bottom of this page.
WHEN THE air quality index (AQI) soared around the Northeast last week in spreading smoke from Canadian wildfires, news reports emphasized immediate potential risks to the heart and lung from fine particulate matter. There is little evidence, however, showing long-term health effects from a few days’ exposure in otherwise-healthy people—aside from a casual comparison of one day’s high AQI levels to smoking about six cigarettes.
Fine particles that come directly from wildfire smoke tend to be “more toxic than other sources of [particles smaller than] PM2.5,” Francesca Dominici, Harvard professor of biostatistics, population and data science told the Washington Post. The reason is wildfires burn everything— which includes “various household materials, such polyvinyl piping and batteries, that produce toxic emissions when combusted.”
(Because so-called “wildland fires” burn plant material, their smoke can be less toxic than fires burning through inhabited structures. Most firefighters use water in their hoses—sometimes with added salts or chemicals used in fertilizer that are poisonous to fish but break down over time; but sprays for Class B fires, such as in jet fuel at airports and oil at refineries, include PFAS (“forever chemicals”) linked to serious human health effects.
Wildfire smoke in lab experiments “causes more inflammation and tissue damage than the same amount of air pollution,” according to Reuters, and “has been linked to higher rates of heart attacks, strokes and cardiac arrests.” Moreover, wildfire smoke lingers in the air for weeks and travels hundreds of miles.
Fine particulates can penetrate deeply into lung tissue, leading to “transient reductions in lung function. . . and may also affect the body’s ability to remove inhaled material such as viruses and bacteria from the lungs,” according to the EPA. In air pollution, particles smaller than PM2.5 come from combinations of airborne chemicals emitted from industries and automobiles—but mostly from coal-fired power plants.
There is no “safe” level of small particulate matter or wildfire smoke exposure, according to Marshall Burke, Stanford smoke pollution researcher. “We see impacts basically starting at zero.”
Last week’s AQI numbers sent DC into “Code Purple” (AQI scores from 201 to 300) indicating risk to everyone—and closing the National Zoo as well as postponing a Nats baseball game. In New York City, numbers soared into “Code Maroon” with AQIs in the high 400s —considered “hazardous for everyone”—briefly ranking it number one on the world’s most polluted cities list, above the usual high-scorers in India and Pakistan.
“We haven’t seen something like this with smoke ground level in over 10 years,” said local DC-area WTOP News meteorologist Eileen Whelan. Ground-level smoke is notably the big offender—meaning that even when skies appear ghastly orange or murky brown, smoke may be too high to create serious health risks.
In DC’s average AQI, however, the most villainous offender is ground-level ozone, which has earned the city an F —with fine particle pollution considered acceptable on a 24-hour basis but with regular spikes that exceed guidelines. Ground-level ozone comes from the reaction of “precursor pollutants,” such as hydrocarbons and nitrogen with sunlight, causing an AQI number that tends to rise over the course of sunny days. Stratospheric ozone, in contrast, acts as the earth’s sunscreen to help protect against harmful UV rays—but excessive carbon emissions deplete or create holes in this layer.
“I cannot think of many things more frightening,” Elena Kagan wrote last year about the Supreme Court’s decision that loosened coal-industry pollution standards and, to some, indicated the court’s takeover from the EPA as climate decision maker for the country.
“The climate signal is very strong,” Robert Scheller, professor of forestry at North Carolina State University, told the BBC —speaking of climate change’s contribution to wildfire surges of recent years. “We are seeing both a larger area burned, and more severe fires . . . Spring in Canada has been much warmer and drier than usual, creating a tinder-dry environment for these vast fires.”
“Across the [U.S.], the number of people exposed to . . . extreme smoke days has grown 27-fold in just a decade,” writes David Wallace-Wells, author of The Uninhabitable Earth. And “already the health impact of American wildfires is larger east of the Rockies than to the west.” Pointing to what one historian calls “the pyrocene,” Wallace-Wells notes that 10% of the world’s forests rise from Canadian soil, and he quotes writer John Vaillant describing a 1950 Canadian wildfire: with a smoke plume so large it created weird visual effects “including widespread reports of lavender suns and blue moons.”
Blame for the U.S. world ranking of #46 for average life expectancy—79.11 years in 2020—falls on U.S. industries that make it “the world’s largest producer of oil, its second largest producer of gas and its third largest consumer of coal, and also its largest historical emitter by an outrageous margin,” writes Wallace-Wells. The U.S. is “responsible for about twice as much carbon damage already done to the planet as any other country on Earth.”
When AQI numbers are high, recommendations include staying indoors as much as possible; and for outside activities, wearing high-quality N95 or KN95 masks. But I took comfort from surgeon and co-director of the Climate Institute at George Washington University Neelima Tummala’s comment to the Washington Post that “everyone has slightly different responses to environmental irritants . . . Do I want people to be outdoors exercising and doing good things for their mental and physical health? Yes.”
Also comforting to me, after spending time outdoors on two unhealthy AQI days without noticeable health effects was a good friend’s report of the comparison to six cigarettes a day. On a Code Purple DC AQI day, with that number sounding lower than the daily cigarettes we had smoked in our early years, we went ahead with a planned swim that was only slightly shorter than usual—and lovely.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
LAST WEEK’S announcement of Rosalynn Carter’s dementia has highlighted recent news and questions about the condition—as well as the work Carter has done to encourage “society not to fear people with mental illness,” according to the New York Times. At a 1977 international conference on mental health, Carter said, “We must create a climate in which our most vulnerable are accepted. We must start first with them.”
Dementia—affecting about one in 10 adults ages 65 and older in the U.S. —is the umbrella term for symptoms (several of them sometimes occurring simultaneously) of progressive, irreversible cognitive decline that can arise in a handful of distinct conditions. In 2020, Alzheimer’s Disease (AD), the most common cause of dementia—which includes “early-onset” AD in those younger than 65 years—afflicted more than 5 million Americans ages 65 and older, two-thirds of whom were women.
In people under age 65, the most common form of dementia is frontotemporal dementia or degeneration (FTD)—the recent diagnosis for actor Bruce Willis. FTD affects parts of the brain controlling “executive functions” and can impair behavior involving judgment, empathy and foresight. As in Willis’s case, an early symptom of FTD can be progressive aphasia, the loss of ability to express or understand speech.
In patients with Lewy body dementia, balloon-like protein clumps in the brain, not unlike the protein causing the plaques and tangles of AD, can impair brain-cell functioning and cause unusual symptoms, such as acting out dreams while sleeping and visual hallucinations. Vascular dementia—once called “hardening of the arteries”—affects blood vessels and most often appears as slowed thinking and difficulties with problem solving. Another prominent type is “mixed dementia.”
Two new drugs, Lequembi and Aduhelm, made headlines in recent years for temporarily reducing cognitive decline and possibly slowing the progression of AD —the first hope for AD sufferers, in the absence of any treatment. Controversy swirls, however, around both drugs— monoclonal antibodies that target beta-amyloid protein–due to persistent uncertainty about the role of amyloid proteins in AD, which is most strongly linked to age and genetics. In addition, the drugs can produce minimal benefits and cause significant health problems, and each costs more than $25,000/year.
Also developed recently, the “early-detection” PreclivityAD blood test measures beta-amyloid proteins in the brain. Along with other variables including genetic analysis, the test assesses a patient’s amyloid probability score, indicating “the likelihood they had AD or were at risk of developing the disease.” The developer C2N Diagnostics has been testing an updated, better performing version that includes an additional AD marker: tau proteins that form tangles in the brain. Based on PET (positron emission tomography) scans, tau tangles are to date the best predictor of future brain atrophy.
(PET scans remain the gold standard for AD testing but cost $5,000 to $8,000 per scan; while another test analyzes levels of amyloid and tau protein in cerebrospinal fluid but requires a spinal tap and costs about $1,000. PreclivityAD costs about $500, is not yet covered by insurance and is slightly less accurate than the other two.)
With family history high on the list of AD risk factors, genetic testing can detect the APOE variants 2, 3 and 4—of which APOE4 can indicate the highest risk—though the association of any of these with AD remains unreliable. Alternatively, cognitive screening can help reveal early brain impairment, although a 2020 federal panel withheld its endorsement due to a dearth of research on benefits and harms. In addition, cognitive testing produces less accurate results for well-educated people—notably those who have scored high on academic tests—who engage in regular cognitive activities, such as reading, writing, teaching and learning a foreign language.
That chronological age can diverge from biological age has become a point of emphasis in recent evaluations of President Biden’s mental fitness. In people who are active, according to the New York Times, “the brain continues to evolve and some brain functions can even improve —a phenomenon experts called the neuroplasticity of aging.”
In the news just last week: Taking a daily multivitamin “might help slow memory loss in ages 60 and older,” based on results from a large nationwide study. According to the researchers, “Put another way, the multivitamin group was an estimated 3.1 years ‘younger’ in terms of their memory function than the placebo group.” This finding contradicts years of consensus that better bio-availability of crucial vitamins came from consuming them in food (compared with supplements)—especially from fresh fruits and vegetables—and was sufficient to slow cognitive decline associated with low levels of vitamins B1 (thiamine), B12 and D.
Similarly in the case of omega-3 fatty acids, past advice has emphasized consuming healthy foods, notably fatty fish and sardines. On the other hand, the larger quantities of these fats in fish-oil supplements may be more effective at increasing blood flow in areas of the brain concerned with memory and cognition, and clearly work better for people with particular health issues—such as dry eyes, if used alongside other treatments, such as artificial tears.
Risk factors most often linked to age-related impairment are those over which people are considered to have some control, including high blood pressure, high cholesterol and smoking. Also on the list but more challenging to control are traumatic brain injuries—for which falling down is the leading cause—along with diabetes, obesity and depression.
Inflammation is emerging as a primary culprit in most of these conditions—linked to “all known genetic and environmental risk factors for AD,” according to one summary report. As a result, keeping a lid on inflammation-inducing stress ranks high on the list of measures to help prevent or postpone dementia—as are anti-inflammatory medications and diets.
Generally, anti-inflammatory protocols (AIPs) emphasize eating a wide variety of fruits and vegetables, unsaturated fats, minimally refined whole grains, tea, coffee, herbs, spices and oily fish— and avoiding foods such as fatty cuts of red meat, refined sugary foods and beverages and excess alcohol. Sugar is a primary villain, with evidence that fructose provokes many of the brain changes associated with AD.
Topping the list of prescription drugs implicated in symptoms of dementia—for people who take them for longer than a few months—are benzodiazepines, along with anticholinergics that include medications for allergy, depression, high blood pressure and incontinence. While these drugs have side effects that include “confusion, clouded thinking and memory lapses,” studies have not yet proved that they cause dementia; in addition, many people rely on them for health benefits.
Among other difficult-to-control items on the do-not list are levels of noise and air pollution—along with back sleeping, though that may be risky only if linked to disordered sleep and trouble breathing at night.
For me, sugar remains the main dementia-related demon, but at least I can count the teaspoons. Social engagement, on the other hand, is trickier—requiring a balance of time spent with other people along with enough alone time to keep stress levels manageable.
—Mary Carpenter regularly reports on topical issues in health and medicine.
If this post was sent to you by a friend, you can sign up for the newsletter at the very, very bottom of this page.
DC-BASED development expert R.C. was lying on the operating table, ready to receive anesthesia before a vaginal procedure, when suddenly she couldn’t catch her breath—and signaled frantically to medical staff, who raced her off to the I.C.U. Her diagnosis: Takotsubo cardiomyopathy, a kind of heart attack described by University of Chicago cardiology fellow Shirlene Obuobi as a “largely reversible” but potentially dangerous response to stress.
Takotsubo occurs more commonly among women—for whom heart attacks caused by obstructive coronary artery disease (CAD) can also produce different symptoms than for men. In one case, a 61-year-old woman, who ate well, didn’t drink, never smoked and ran half-marathons, complained of nausea and fatigue along with an ache in her right arm. After vomiting, she went to bed and the next morning died of a heart attack.
And patients with chest pain but no artery blockage observable on scans—especially women—often struggle to get physicians’ attention, writes Obuobi. Many women seen in the ER with atypical symptoms receive a diagnosis of anxiety and the advice to go home. Only recently recognized, MINOCA refers to “myocardial infarction with nonobstructive arteries.” In fact, only 15 to 25% of patients reporting chest pain turn out to have a blocked artery.
The effects of intense stress on the body range from serious heart attacks to situational anxiety, the bane of public speakers, and respond to similar drugs, notably beta-blockers. Explains the Mayo Clinic website, stress prompts the hypothalamus to set off an alarm system that causes the release of hormones, such as cortisol and adrenaline, and “communicates with the brain regions that control mood, motivation and fear.”
Cortisol increases the body’s use of circulating glucose and raises energy levels, while excess adrenaline can speed up the heart rate and elevate blood pressure—and in some cases, lead to the shortness of breath, sweating and dry mouth that arises in situations such as stage fright. Adrenaline and other stress hormones overwhelm or “stun” the heart cells, causing Takostubo cardiomyopathy, also called “broken-heart syndrome.”
Massive amounts of adrenaline cause the heart to balloon, weaken and “quite literally” give out. Adrenaline can narrow the small arteries that supply the heart with blood or bind directly to heart cells, which can prevent the heart from beating properly. Both emotional and physical stress—such as asthma and low blood sugar—can cause broken heart syndrome. But, explains Johns Hopkins heart failure specialist Ilan Wittstein, “up to 30% of patients have no identifiable trigger at the time of their initial symptoms.”
The risk of developing Takotsubo increases five times after the age of 55 . . . and the vast majority of patients are post-menopausal women,” according to the Hopkins site. “It is believed that because the female hormone estrogen helps to protect the heart from the harmful effects of adrenaline, women become particularly vulnerable to the effects of sudden stress as they grow older and their estrogen levels decline.”
“Heart disease is the leading cause of death for women in the United States and can affect women at any age,” according to the CDC. Over 60 million women (44%) in the United States are living with some form of heart disease [and in] 2020, it was responsible for . . . about 1 in every 5 female deaths. Research has shown that only about half (56%) of US women recognize that heart disease is their number 1 killer.”
What women in particular should do is “pay attention to any symptoms above the waist, which means above the belly button, that are new to you,” Barbra Steisand Women’s Heart Center director C. Noel Bairey Merz told the Washington Post. For talking with medical staff, Obuobi advises being specific when describing the pain, starting with what it feels like and where it occurs. Heart attack patients often describe “pressure-like squeezing or heavy” sensations that last several minutes and worsen with exercise; and cardiac pain that moves up the jaw or down one arm.
Also more common for women, signs of a heart attack can include new discomfort or pain occurring in the neck, jaw or throat, or in the upper back or abdomen —as well as indigestion or heartburn; dizziness or shortness of breath; and profound fatigue—with symptoms that linger and intensify over a period of hours. Sharp pain, on the other hand, especially if it worsens with exercise, is less likely to be caused by a heart condition.
And while heart attacks occur at any time of day, any pain that arises early in the morning most often signals a different problem: microvascular dysfunction or spasms in arteries feeding the heart, which results in depriving the heart of oxygen. Heart spasms can occur in response to cold weather or other stressors, or spontaneously, but do not involve adrenaline and require different treatment from other heart conditions.
To combat adrenaline’s effects on the heart—from heart attacks to situational anxiety—beta-blocker drugs are among the most-prescribed medications in the U.S., used by some 30 million adults. The FDA has approved beta-blockers for heart-related conditions such as high blood pressure or irregular heartbeat; doctors also prescribe them “off label” for people who struggle with anxiety—most often the kind that arises in specific situations like public speaking, rather than for those living with a diagnosed anxiety disorder.
R.C. received a prescription for beta-blockers after her Takotsubo incident, while I take them before I need to speak in public. During a recent two-week period of almost daily presentations, I believe beta-blockers helped reduce my worst reactions—dry mouth that can make it hard to talk and sometimes shortness of breath and dizziness.
While the body’s stress response is usually self-limiting, high cortisol levels can continue to curb functions that would be nonessential or harmful in a fight-or-flight situation, which can result in altered immune responses. For me, a little cut or scratch that takes longer to heal is a clue that I haven’t entirely recovered from a stressful period —and a signal that I should try to get more sleep.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
AT AGE 25, the writer Flannery O’Connor became ill with lupus, forcing her to move from an independent literary life in New York back home to the middle of Georgia and back in with her mother. Lupus (systemic lupus erythematosus) and multiple sclerosis (MS) are two autoimmune diseases with a lot in common that have afflicted famous young female artists.
Known as “relapsing-remitting disorders,” the course of each involves flares of symptoms followed by remissions. Especially during remissions, lupus and MS fall into the relatively recent category of “invisible” illnesses or disabilities—which can include everything from ADHD to cancer. As posted on the Invisible Disabilities website: “People are parking in an accessible parking space with a placard, but they look fine. I wonder if that driver has an invisible disability.”
“The category of invisible illness, which means exactly what it sounds like—an illness or disability not immediately apparent—is growing sharply in America,” writes Mireille Silcoff in a New York Times essay on the invisible effects of a head injury, inspired by the case of retired optometrist Terry Sanderson. Suing actress Gwyneth Paltrow for damages following “a ski collision he said was her fault,” Sanderson acknowledged that he had continued to travel and do Zumba, and he lost his case.
“Through the wonders of medicine we’ve become great at turning life-or-death illnesses, like diabetes, heart conditions or certain forms of cancer, into chronic conditions that can often be lived with,” according to Silcoff. “At the same time, diagnoses of hidden diseases like Crohn’s or fibromyalgia are becoming increasingly common—as is long Covid, which on its own might have affected as many as 23 million Americans.”
Both lupus and MS occur more commonly in young women, from the late teens to early 40s; and symptoms for both can include muscle and joint pain, fatigue and neurological deficits. Most sufferers of both are able to lead normal lives between flares, and have typical lifespans.
And both conditions have “clinical diagnoses” in the absence of a lab test or imaging that provides confirmation. The difficulty of a definitive diagnosis is a burden for many sufferers of the more than 80 autoimmune diseases—which can also have confounding symptoms. Muscle aches and fatigue, for example, can appear similar in more than one autoimmune disease as well as in many other illnesses.
The parts of the body affected by different autoimmune diseases usually determines the symptoms—from alopecia areata that causes hair loss, to type I diabetes that destroys the pancreas. And the causes of most autoimmune diseases include genetic components as well as triggers that can include viruses and environmental factors. According to medlineplus, “if you have one autoimmune disease, you are more likely to get another.”
Most challenging for many sufferers is the unpredictability of relapses, which “can make you angry—and for good reason [that they] don’t follow the rules and they don’t play fair,” writes Erica Jacques on verywellhealth. “It can be frustrating, especially, when your symptoms recur when you’re doing everything right, or remit when you’re doing everything wrong . . . with MS, anger can be caused by changes in the brain as well [and] autoimmune diseases can produce in your mind a deep feeling of insecurity.”
Until recently, corticosteroids offered the primary relief for sufferers of these conditions by tamping down the immune system—but over time such dull weapons also damage bones and organs. Newer, better-targeted biologics—biologically engineered proteins—can get the immune system working normally “by turning certain cells and proteins of the system up or down,” according to verywellhealth.
Because MS affects the nervous system and brain, early signs can include double vision, numbness and tingling and problems with balance. Cellist Jacqueline Du Pre, the subject of the film Hilary and Jackie, lost sensation in her fingers that forced her to stop performing at age 28. She began behaving so erratically that her sister Hilary said later, “the Jackie I knew and loved died years before her actual death in 1987.”
With lupus, an out-of-whack immune system causes inflammation and damage to healthy connective tissue throughout the body —in the skin, joints, kidney, heart, and lungs—with the nervous system and brain less common targets. Early symptoms of lupus are usually migraine headaches, rashes and joint pain.
When Flannery O’Connor’s lupus first appeared in 1950, corticosteroids were new, and early difficulties controlling the dosages led to weakness in her bones. Her health deteriorated until she died from kidney failure at age 39. In the end, however, she was grateful to spend her last years in Georgia, where her mother Regina brought daily reports from the town gossip and, as Flannery said, the sounds of the South, mostly the southern way of speaking “build up a life of their own in your senses.”
Many people struggle with invisible difficulties, including mental health issues like severe anxiety and panic attacks. A “disability,” according to medicalnewstoday, “makes it more difficult for the person with the condition to do certain activities (activity limitation) and interact with the world around them (participation restrictions).” As Silcoff noted in the New York Times, “A man can have a life forever altered by a concussion. And he can also Zumba.”
Peripheral neuropathy, or diminished sensation, in my legs and feet can cause me to lurch and veer when I walk, but it’s not a disability for me. And the symptoms are not invisible but rather misleading: As MS sufferers notoriously report, wobbly walking looks like drunkenness. A few incidents with people leaning in close to check for alcohol on my breath helped convince me to give up drinking, but these also gave me greater awareness of the possibility of invisible disabilities in almost everyone.
—Mary Carpenter regularly reports on topical subjects in health and medicine.
“SQUAMOUS cell carcinoma (SCC) is a life-threatening type of skin cancer,” according to Harvard Health—and not the benign problem that many people think. In the first episode of “New Amsterdam”—a TV series based on the true story of Bellevue physician Eric Manheimer, called Max in the show—the diagnosis came up in ominous tones accompanied by “have you told your wife?”
While most SCCs occur on skin, making them easily visible and often simple to remove in their entirety—those arising inside the body can become more complicated, with a recent case requiring complete jaw reconstruction.
But even when squamous cell carcinomas is on the skin’s surface, diagnosis and treatment are not always straightforward. For former DC area political consultant R.F., his medical team surgically removed SCC lesions—but afterwards shared biopsy slides with two other cancer centers. The team was concerned about the possible presence of spindle cells—specialized cells that are tricky to detect and can indicate the cancer may have penetrated to a deeper level and could be life-threatening.
SCC is the second most common form of human skin cancer—with at least 200,000 to 400,000 new cases of SCC expected each year in the US, according to the American Academy of Dermatology. For comparison, the more worrisome melanoma affects nearly 100,000 Americans a year, with survival rate at five years around 94%—unless it spreads to other areas of the body, notably the lymph nodes.
The most common skin cancer, basal cell carcinoma (BCC), was the diagnosis for First Lady Jill Biden’s skin lesions, removed in early January—and also for lesions removed from Nancy and Ronald Reagan, and George H.W. Bush, according to the Washington Post. Occurring in cells that form the deepest layer of the skin, basal cell carcinoma causes eight of every 10 skin cancers; while it can be aggressive, the lesions rarely metastasize.
“It’s a matter of exposure,” states the mdanderson site, explaining why most skin cancers occur on the head and neck. “Because those are the areas most often left uncovered—so they get the most exposure to UV radiation.” The five-year survival rate for SCC is 99%—although the number drops to about 50% for throat SCC that has metastasized.
For his squamous cell carcinomas, R.F. had Mohs surgery, performed in stages that involve slicing thin layers of skin and examining the cells while the patient waits—and the surgeon continues slicing until cancer cells are no longer present. Also called Mohs micrographic surgery, the procedure includes removal of a margin of cells around the cancerous spot, according to the skin cancer foundation, and allows for “the removal of all cancerous cells for the highest cure rate while sparing healthy tissue and leaving the smallest possible scar.”
Also used to treat First Lady Biden, Mohs is “the most effective technique for treating many BCCs and SCCs,” according to the Skin Cancer Foundation. Physicians often recommend Mohs for skin cancers that are large or aggressive, have edges that are hard to define, occur in certain areas where tissue is thin such as the scalp, or when cancer involves mucous membranes, such as on the lips. For more advanced cases, physicians add radiation or chemotherapy.
Squamous cells line the surface of the skin as well as the interior surfaces of the mouth and stretch down from the oral cavity into the esophagus and lungs—as well as into the cervix, anus and bladder. As surface-lining cells change, tumors can form in the glandular tissue that lines internal organs, such as the lungs, where they are more commonly labeled adenomas and can also become malignant.
UV radiation is the main cause of head-and-neck SCCs on the skin’s surface, which usually begin with suspicious areas that can be tender, raised or higher than the surrounding skin—and don’t improve after several weeks. In some cases, SCC begins with ulcerated sores inside the mouth or a painless lump in the neck that indicates a swollen lymph node. Human papilloma virus may be another cause of SCC in the throat.
For Eric Manheimer, squamous cell carcinoma kept him out of work for six to eight months. In his 2012 book Twelve Patients, Manheimer describes his treatment using “a radiotherapy mask that required him to be bolted down to the table,” according to the New York Post. “It’s a computerized program…the rads are built exactly to your tumor so you can’t move your head at all. It’s a mask molded to your face.” R.F.’s recent journey with squamous cell carcinoma began when he noticed two suspicious spots on his head, which were sore to the touch. During the Mohs surgery, his medical team concluded that they had excised “all traces” of SCC—and follow-up scans over the next five months have been clear. According to R.F., the team “removed any underlying spindle cells— if that’s what they were.”
Recently R.F. learned that his cousin and son had similar skin cancers in locations similar to his. While about 10% of melanomas may be linked to family history, SCC is “generally not inherited, it typically arises from mutations in the body’s cells that occur during an individual’s lifetime…called a somatic mutation,” according to the National Library of Medicine’s MedlinePlus site. But “rarely [SCC] is found in several members of a family [with] inherited disorders that increase the risk of multiple types of cancer.” At last week’s CT scan, R.F. received the good news that he can wait six months before his next visit. His wound continues to require regular care, in part because he chose not to have skin grafts that can help cover the wound but have been linked to increased risk of infection. He urges everyone to get regular dermatologist body scans and pay attention to anything unusual occurring on the skin. Last week, he returned to his weekly swims, wearing “a very tight cap”—and was back on the tennis courts, with lots of sunscreen, of course.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
“Too much shellfish (oysters, of course) and alcohol (festival life!), and not enough water might have exacerbated this bout,” emailed Europe-based film critic C.M. after waking up on her final morning in New Orleans for the Tennessee Williams Festival with the excruciating pain of gout. What could have helped: avoiding beer, organ meat and tuna; also, drinking coffee and eating cherries!
Only after an ER nurse asked about gout did C.M. remember her diagnosis from years before, but because that had been for a swollen big toe, the classic location for gout, she hadn’t made the connection when intense pain struck her ankle. Also, as she noted, “it’s more common for men to have gout—and I’m not overweight, or a drinker and stopped eating liver.”
Gout is the most common form of inflammatory arthritis and more prevalent now than ever, according to Science Daily, “affecting more than 10 million people in the United States or approximately 5 percent of the adult population.” Still, many Americans think of gout as a disease from a bygone era and one that afflicted “the rich and royal, including American historical figures such as Benjamin Franklin and Thomas Jefferson.”
Postmenopausal women are susceptible to gout because they lack the protective effects of estrogen—although the attacks occur most often in middle-aged and older men. One risk factor for gout is obesity, and its increase in the U.S. population may help explain its rising prevalence. In addition, diuretics that are increasingly prescribed for high blood pressure can lead to dehydration—a major trigger of gout attacks.
What causes the sudden, rapidly increasing pain that signals a gout flare is the accumulation of uric acid—either when too much uric acid is synthesized in the body or when the removal capacity of the kidney is compromised, according to medical.net. Uric acid results from the breakdown of a chemical called purine —which is present naturally in the body and occurs in high levels in animal proteins, such as pork, red meat, shellfish and oily fish. In addition, alcohol reduces the metabolism of uric acid and can contribute to dehydration.
The buildup of uric acid in the form of urate creates “needle-shaped crystals in and around the joints, usually starting in the foot,” according to Science Daily. Flares occur when the body starts reacting to the deposited crystals, resulting in joint swelling, severe pain and tenderness. Patients suffering from gout for a prolonged period can form nodules of uric acid around the joints, called tophi, and over time gout can progress to “chronic joint damage.”
Besides obesity, risk factors for gout include diabetes, kidney disease, chemotherapy and family history. Of genetic mutations discovered to date, one affects the circulating levels of lubricin, which lubricates and protects joint tissues—and may one day be used as a biomarker for tracing a patient’s risk of developing gout. Another mutation slows the excretion of uric acid, which results in its accumulation in the blood, although high blood levels, called hyperuricemia, are an unreliable indicator of gout.
Diagnosis of gout usually relies on blood and urine testing. The drug allopurinol, used for long-term treatment of gout, can help prevent flares. But for the intense pain of attacks, therapies include glucocorticoids, such as prednisone, and nonsteroidal anti-inflammatory drugs (NSAIDs). Another option is colchicine, a chemical found in many plants—notably wild saffron or autumn crocus—and described for pain and inflammation in the oldest Egyptian medical text, circa 1550 B.C. Investigators who looked into using colchicine for treating Covid found it ineffective.
C.M. had taken allopurinol briefly after her big-toe gout flare, but in New Orleans, NSAIDS quickly alleviated the pain—and she drank more coffee. C.M. wrote, “It was a relatively minor inconvenience…more worrisome than anything else, until I found out what the problem was”— and she hobbled her way through the rest of her trip around the United States.
In my family’s house, gout came up often at the dinner table, because my stepfather who had rheumatoid arthritis also had gout. For someone whose arthritis had caused such severe disability that many of his joints were fused—including his unbending fingers—my stepfather talked about the excruciating pain of gout attacks if anyone suggested one of the foods or drinks believed at the time to trigger flares. Vegetables high in purine, such as asparagus and spinach, were forbidden, although these have since been shown to have no effect on the risk of gout or gout attacks.
We never drank red wine—only white–although “moderate consumption” of either is now permitted. And we never had organ meats or shellfish. But while the current recommendation is to cut back on saturated fats, our several-times-a-week, most-popular, warm-weather meal consisted of summer corn with an enormous steak, grilled black and served very rare— served only with white wine, rather than the better accepted pairing with a full-bodied red.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
LAKE TAHOE medical editor P.D. had spent months digging her car out from under dozens of feet of snow when she flew to Italy—to travel and take a food tour in Puglia. A week into her trip, P.D., who is in her late 70s and fully vaccinated, developed a cough and tested positive for Covid. She then quarantined in her Bari hotel room for five days.
Covid is still out there—though symptoms are becoming less severe among people under age 65 and the number of weekly deaths due to Covid is declining. Last week the FDA announced plans to authorize a “spring shot” for older and immune-compromised adults—of the bivalent vaccine designed to protect against the omicron strain and its subvariants—to help counter waning immunity.
“An acknowledgement of the virus’s continuing risks to vulnerable people whose immunity might be sagging months after a previous inoculation” is how the New York Times describes the FDA’s plans “to authorize…without explicitly recommending [the additional dose], a stance that emphasizes the discretion of patients and their health providers.”
People over age 50 should be offered the chance to get a spring booster, Michael Osterholm, director of the University of Minnesota’s Center for Infection Disease Research and Policy, told STATnews. Osterholm noted that in the second half of 2022, 97% of people who died from Covid in this country were age 50 and older.
Having a spring shot can help bridge immunity gaps until late summer when a new reformulated vaccine is expected. In one study of patients deemed vulnerable to severe Covid, protection against infection declined from 61% in the first months after the original vaccine to only about 16% by the sixth month, according to Washington Post editorial writer Leana Wen —who noted in March that “for months the single-most common question I have received from readers has been about when they can get a second bivalent dose.”
Boosting brain health is another good reason to get the spring shot. “All types of vaccinations were associated with a trend toward reduced dementia risk,” according to a multicenter study by Chinese researchers. Comparing dementia risk in vaccinated versus unvaccinated populations, their analysis found vaccinations were associated with a 35% lower dementia risk.
Vaccinations against flu, pneumonia and shingles appear to offer protection against Alzheimer’s and Parkinson’s diseases, the most frequent forms of age-related neurodegeneration. According to neurologists Avram Bukhbinder, now at Mass General, and Paul Schultz at University of Texas, Houston—who looked at the effects of flu vaccination on a large nationwide sample of adults age 65 and older, “People who received at least one influenza vaccine were 40% less likely than their non-vaccinated peers to develop Alzheimer’s disease over the course of four years.”
Worries about symptoms of “long-haul” Covid—disabling fatigue, cognitive problems, pain and shortness of breath—may be the reason many eligible people get the “spring booster. Among four to seven million people who have had symptoms of Long Covid, 79% report having limitations to daily activities and 27% say those limitations are significant, according to the Kaiser Foundation website. The rate of Long Covid among people who have had the infection remains as high as 28%—although that is a decline from 35% in January 2023; and more than half of those who had Long Covid are no longer reporting symptoms.
Paxlovid—the antiviral treatment recommended for nonhospitalized adults and some pediatric patients with Covid who are deemed at high risk of disease progression—appears to help both to prevent Long Covid and to treat the long-term symptoms, according to TIME magazine. And in recent research, the diabetes drug Metformin appeared to stop the SARS-CoV-2 virus from replicating, explains University of Minnesota medical school researcher Carolyn Bramante—which may help prevent severe disease as well as long-term complications of Covid. The possibility of innate immunity to Covid—the apparent resistance of some people to infection despite known exposure to the virus—is the focus of the U.S.-led Covid Human Genetic Effort. After research failed to support early theories linking Covid-resistance to blood type, the search is now on for an inherited mutation in the cellular receptors or enzymes needed for the virus to gain entry to the cells. Another explanation could be a mutation in a gene involved in the immune response to infection, as with genetic mutations that bestow resistance to other infections like HIV and norovirus, the so-called winter vomiting bug.
After P.D. of Lake Tahoe managed to avoid Covid infection over three years of the pandemic, she thought she might have some kind of innate resistance and began to relax precautions, such as masking. All that changed with the Italian experience—and hearing about that convinced me to be even more vigilant. For whatever reason I have managed to avoid Covid infection to date, I think the spring shot cannot come soon enough—with high hopes that it will boost my resistance to the virus and help me avoid the dreaded Long Covid and in the process even benefit my brain.
—Mary Carpenter keep us updated on the continuing risks of Covid 19.
Taping your mouth shut for sleeping came up in Mary Carpenter’s 2021 post on James Nestor’s book, Breath the New Science of a Lost Art. But since a November 2022 New York Times article “Can a Piece of Tape Help You Sleep?” continues to inspire readers’ comments–522 as of last week–and becoming a practitioner and true believer herself—she has written an update:
“A MORE efficient, effective way of breathing” is how Stanford University “voice and swallowing specialist” Ann Kearney described nasal breathing to the New York Times—compared to breathing through the mouth. “Sleeping with your mouth agape may cause you to wake up with a dry mouth, which can contribute to cavities, bad breath, a hoarse voice and dry, cracked lips.” And in small studies, nasal breathing has helped alleviate snoring in people with mild obstructive sleep apnea.
Nasal breathing “humidifies and filters the air, and activates the lower lungs, letting you take deeper, fuller breaths. It can also help your body relax as you ease into sleep,” says Kearney. USC pulmonary and sleep medicine specialist Raj Dasgupta explained that breathing through the nose causes the sinuses to naturally produce a gas called nitric oxide, which flows…to the lungs and into the blood. It can widen blood vessels to improve blood flow and lower blood pressure, and can create an overall calming effect.
“Despite its recent popularity, mouth taping has not been extensively studied,” cautions the Times article, which includes suggestions to use a light, skin-friendly tape like surgical tape along with warnings that people with sleep difficulties should see a sleep specialist. Kearney and others caution that anyone struggling to breathe through the nose—if you can hear yourself when you attempt to nasal breathe—should not try mouth taping.
“I read somewhere that when women are ready for sleep their brain is still maybe 80% active so they can happily chat away with pillow talk for a long time whereas when men are ready for sleep their brain is maybe 15% active and unable to enjoy such pillow talk,” writes one commenter. “If I’m ready for sleep and milady engages me in pillow talk, it will actually wake me up again, leaving me unable to wind back down to sleep-readiness for maybe 90 minutes. So I hate that—and taped lips are a beautiful out ‘sorry can’t speak’— zzzzzz—works for me!”
(“Multiple studies have shown that women fall asleep faster than men,” states the Sleep Foundation site. And according to the Wall Street Journal, women take an average 9.3 minutes to fall asleep, while men take 23.2.)
“Using a cheap supermarket bandaid horizontally to tape my lips closed” is this commenter’s recommendation. Writes another, “All I had was some type of duct tape, it’s not as bad as reported. . .it feels like a helpful thing. . .and I don’t wake myself up snoring.”
“I love the results—I’ve not had a blocked nose for a long time,” writes a daytime mouth taper. “I also exercise while nasal breathing (a face mask will hide the tape!) . . .mimics high altitude training, which increases the body’s ability to use the O2 it has.”
“Article got it wrong,” writes a complainer. “You don’t ‘tape your mouth shut.’ Rather you place a bit of tape vertically across the lips to ‘remind’ you not to open your mouth. If you did need to open your mouth you certainly could do so . . .we don’t need the usual ‘experts’ to weigh in on this easy and mild practice.”
“Seems to me this is an extremely risky practice,” writes a worried commenter. “If you develop a condition overnight that blocks your nasal passages. . .do you really want to be unconscious for eight hours with one of your primary breathing passages sealed shut?”
“My low-level anxiety, precursor to claustrophobia, kicks in,” adds another, despite being a “long-time” user of a CPAP machine. “Also what if young children see their parent with mouth taped shut…might think it would be fun to tape younger siblings mouth shut.”
The popularity of Nestor’s Breath to date has boosted sales of its recommended products—from the most inexpensive sleep strips to very pricey, personally fitted mouth retainers. In his self-improvement journey as a “pulmonaut,” Nestor links nasal breathing to possibilities for improvement in almost all bodily functions. And naturopath and healer Andrew Weil, quoted in the epilogue of Breath, writes, “If I had to limit my advice on healthier living to just one tip, it would be simply to learn how to breathe better.”
Dry mouth was my original reason for mouth taping—after reading Nestor’s book—which at its worst caused my tongue to swell to the point that it impeded talking and eating. While taping my mouth shut seemed weird at first, I became a convert once my trusted physical therapist admitted doing it every night. As one commenter suggested, more as a reminder than a tight covering, I use a small strip of surgical tape that connects the philtrum (the midline groove in the upper lip) to lower lip. It’s thin enough (1/8 of an inch) that I can cough or even pop in a cough drop when needed.
Since starting to tape, I’ve never had a repeat of the severe dry mouth. To date, the biggest drawback occurred one day when I failed to remove all the sticky stuff—acrylate adhesive—in the morning, which proceeded to collect dirt throughout the day—with not one of the many people I encountered letting me know there was a big black blob hovering on my upper lip.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
A FEMALE patient appears too dejected to speak with medical personnel until finally one physician observes the patient take an elegant fountain pen from her purse. The physician remarks on the pen, saying she recently received a nice one for a gift. The patient asks about the gift pen, enthuses about that particular pen, mentions her membership in a club for fountain pen enthusiasts, and bursts into tears—and talks about how upset she is about a death in her family.
Broadly, “narrative medicine” refers to bridging the “isolation of doctor and of patient [using stories] to help us know the patient outside of one moment in time,” explained Suzanne Koven, primary care physician and “inaugural writer in residence” at Mass General Hospital. Author of Letter to a Young Female Physician, Koven spoke on the panel “Health and Illness Narratives: Harnessing Medical Memoir to Impact a Broken System” at the recent AWP (Associated Writing Programs) conference in Seattle.
For patients, creating a narrative—rather than listing symptoms without context—can help medical personnel seeking to treat them. More commonly, “narrative medicine” refers to formalized training for physicians to deepen their capacity for understanding their patients. Another goal is to help physicians heal themselves—from the stresses of coping with traumatic medical issues, such as during the pandemic, as well as of never-ending work and time pressures, which in turn create the greatest barriers to empathy with their patients.
Evidence-based medicine has the aim of “integrating the experience of the clinician, the values of the patient and the best available scientific information to guide decision-making about clinical management,” writes geriatrician Caroline Fife at Baylor College of Medicine in Houston. But physicians can lose sight of this goal in “the incessant drum beat of the hierarchy of evidence.”
“Can it be that learning how to enter the narrative worlds of our literary texts and visual images can deepen our awareness of patients’ subjective lives? Can it be that the humanities not only humanize but make more effective the care we provide to others? It can be,” asserts Rita Charon, who coined the term “narrative medicine” and founded the Program in Narrative Medicine at Columbia University in 2000. In 2018, Charon gave the National Endowment for the Humanities (NEH) prestigious Jefferson Lecture.
“The effective practice of medicine requires narrative competence, that is, the ability to acknowledge, absorb, interpret, and act on the stories and plights of others,” Charon wrote in JAMA. Learning how to read closely and analyze texts— from illness narratives such as Tolstoy’s “The Death of Ivan Illich” to Henry James on the “great empty cup of attention”—can help physicians develop empathetic listening skills to better understand and connect with patients.
To counter stereotypes about “elder patients,” second-year students at New York’s Weill Cornell School of Medicine hear talks from over-80-year-old women—in one case, describing a sexual relationship with a younger man; and in another, a physician’s dismissive “at your age [people have less energy]” response to what was in fact a low-grade infection requiring treatment. In narrative medicine reading groups, one physician admitted to having no training in how to treat patients with disabilities, while another confessed to being judgmental about patients undergoing bariatric surgery.
While lack of time is the reason most often given for physicians failing to engage patients, old clichés reflect important barriers—that physicians “see what they know” and “know what they see.” For orthopedists trained in doing surgery on joints, for example, looking at scans of joints riddled with arthritis tells them that those joints require surgery—with the risk that they focus on the wrong joints or on the wrong cause entirely for a patient’s distress.
For patients wishing to tap into the resources of narrative medicine, one suggestion is to begin an appointment by telling the physician you have a specific number of topics/questions (best to keep that number below five) and then create a storyline for your complaint. Actually writing down a numbered list beforehand can help, so that a busy physician sees you moving down the list. For my knees, which appear arthritis-riddled on scans, I could say, “My knees are not painful but my gait became abnormal after I had Lyme disease, which caused peripheral neuropathy, and that means I have trouble feeling my feet.”
And Lyme disease gave me my first lesson in storytelling. When I couldn’t convince my doctor that my muscle pain deserved her attention, I created and then rehearsed a story: “I go to bed at midnight, but I can only sleep for half an hour before the pain wakes me up, and for the rest of the night, I pace up and down in my nightgown on a public beach, and I watch the clock until I can take the next dose of Advil.” After that, my doctor prescribed doxycycline and ordered tests for Lyme disease—which came back positive a few days later.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
MyLittleBird often includes links to products we write about. Our editorial choices are made independently; nonetheless, a purchase made through such a link can sometimes result in MyLittleBird receiving a commission on the sale. We are also an Amazon Associate.
THE SYMPTOMS U.S. diplomats around the world experienced—known as the Havana syndrome—have no biological basis, according to the latest report. As a result, these symptoms, including severe headaches and vertigo, have become the most recent evidence of psychogenic, or psychologically based, factors playing an important role in physical disease. In addition, researchers at Harvard’s Program in Placebo Studies (PiPS) recently revealed involvement of psychogenic factors in the side effects experienced by Covid vaccine recipients.
Ever since Freud first wrote about “conversion disorders,” which include physical symptoms caused by fear, anxiety and other stressors, adding the word “psychogenic” to a diagnosis can make patients feel their complaints are not being taken seriously. The Harvard PiPS program is working to change this perception, in some cases using MRI and PET scans to document the body’s responses to placebo treatments—concluding, for example, that “placebo needles produce better pain relief than placebo pills but . . . placebo pills are better for insomnia.”
All disease is “biopsychosocial,” asserts Suzanne O’Sullivan in her book The Sleeping Beauties: “Havana syndrome was a powerful sociopolitical issue.” The title’s sleeping beauties refers to “resignation syndrome,” diagnosed in refugee children in Sweden who fell into coma-like states —which automatically qualified a family for asylum, and which later resolved when asylum was granted.
The “anomalous health incidents” reported by more than 1,000 U.S. diplomats around the world, first in Havana, included temporary loss of hearing and other symptoms similar to those of traumatic brain injury, according to Politico. The latest investigation failed to detect any biological evidence of these symptoms—or of the deployment of weapons, such as damaging electrical waves, by a foreign adversary.
But the seven government agencies involved in the Havana syndrome investigation had “varying levels of confidence” in the conclusion—and their conclusion avers only that involvement of a foreign adversary is “very unlikely.” Meanwhile, the Pentagon continues to test weapons that could cause these symptoms and is also working to develop weapons that could defend against such attacks.
Difficulties arise because the workings in the body of psychogenic factors are still “not well understood,” according to the Harvard Medical School news site. For the placebo effect, “some theories point to [patients’] expectations as the primary cause and others argue that nonconscious factors embedded in the patient-physician relationship automatically turn down the volume of symptoms.” Placebo treatments work most effectively for symptoms modulated by the brain, such as pain, stress-related insomnia, fatigue and nausea. The PiPS team has found that common chronic conditions improve when medical personnel fully disclose placebo treatment— called “open label” or “honest” placebo—for example, dispensing sugar pills in bottles clearly labeled “Placebo”—along with clear explanations to patients about the brain’s role in their symptoms.
“Functional disorders appear to hijack the normal neurological mechanisms by which we experience our body,” according to the New York Times. So-called “cheerleaders’ disease” that affected several groups of U.S. high school girls, for example, included Tourette’s-like tics and movements.
The nocebo effect, on the other hand, “occurs when a person experiences unpleasant responses after receiving a treatment that has no pharmacological properties,” according to the Harvard site. In the PiPS meta-analysis of 12 Covid vaccine studies, close to one-third of participants who received a placebo reported at least one adverse event.
The most common complaints in the placebo group were the “nonspecific symptoms like headache and fatigue—which we have shown to be particularly nocebo sensitive,” according to PiPS founder Ted Kaptchuk. Casting doubt on this gold standard of medical research, PiPS investigator Julia Haas noted that “adverse events after placebo treatment are common in randomized controlled trials.”
In addition, for PiPS study participants who received the active vaccine, greater anticipation of problems after a first dose can help explain the higher rate of adverse effects reported after their second dose. Altogether, according to the site, “the team’s analysis suggested that nocebo responses accounted for 76% of systemic adverse events in the vaccine group.”
“Informing the public about the potential for nocebo responses [to the Covid vaccine] could help reduce worries about Covid-19 vaccination, said Kaptchuk. And understanding this reason for side effects—which have been a major concern among antivaxxers—“might decrease vaccine hesitancy.”
“Medicine is based on trust,” according to Kaptchut. Ongoing PiPS studies are investigating the role of patients’ expectations as well as of the patient-provider relationship in clinical responses to acupuncture, both sham and genuine, for osteoarthritis of the knee and in the treatment of chronic low back pain—with objective measurements of sham treatment effects using fMRIs and PET scans. For asthma patients, one PiPS study found that “placebos can have effects similar to powerful medications, as measured by a self-appraisal of subjective symptoms, yet have no detectable effect on objective pathophysiology.”
An “exceptionally high rate of placebo response” occurs with treatments for depression,” according to PiPS research. Antidepressants have worked well for me: I have tried only once to wean myself off , with unpleasant and challenging results. I continue to be grateful for these antidepressants—and as a result for the placebo effect, whatever role it plays.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
MyLittleBird often includes links to products we write about. Our editorial choices are made independently; nonetheless, a purchase made through such a link can sometimes result in MyLittleBird receiving a commission on the sale. We are also an Amazon Associate.
SPENDING four days at Atman, a Jamaican psilocybin retreat, was emotionally moving, spiritually rewarding and fun for retired D.C. area rabbi L.M. Most important to L.M.’s positive experience were the retreat’s guides, who “provide a ‘container’ for the psilocybin [magic mushroom] experience. You want that to be healthy and good.” (With psychedelic drugs not yet legal in the U.S., retreat organizations offer experiences solely outside the country.)
In his new memoir, Spare, Prince Harry talks about using mushrooms to help with prolonged grief after the death of his mother “therapeutically, medicinally,” writes Dana G. Smith in the New York Times. Smith explains, “Scientists think that psychedelics work in two ways: through their chemical effects on the brain and the subjective experiences a person has while on the drugs.”
With trust a crucial factor for those like L.M. seeking a psychedelic experience—for most people, out of curiosity but also with some hope of having the transcendent experiences described by others—L.M. chose Atman from the site created by How to Change Your Mind author, Michael Pollan.
“The opposite of spiritual is egotistical,” Pollan has explained in interviews. “To the extent that you can diminish the role of the ego, you become a more spiritual person—more connected, less defended.” The ceremonial aspects of Atman’s psilocybin experience impressed L.M., such as when the guides suggested beforehand that participants might want to place an “offering” or meaningful object at the center of the room.
To this “altar,” L.M. added his tefillin, two small leather boxes containing sections of Torah connected by a leather strap, which are worn on the body close to the heart and the brain. For L.M., tefillin “symbolize the human desire…to be One with the intelligence governing the universe, to lose one’s ego and experience the creative intelligence at the basis of all existence.”
Also reassuring to L.M. was that his guide had a PhD in psychology and was involved in clinical research and that the nine participants included four M.D.’s. For each session, the Atman retreat provides three guides plus two other “team members,” with a maximum group size of 12 participants.
Psilocybin and ketamine are the two psychedelics, among a host of those currently being studied, that are “leading the way,” according to Field Trip Health. While the two compounds overlap in their effects and fall under the umbrella term psychedelics, psilocybin belongs in the category of hallucinogens while ketamine originated as a dissociative anesthesia drug.
“Psilocybin and other psychedelics are thought to promote neuroplasticity, a rewiring of the brain that gives patients fresh perspectives on longstanding psychiatric problems,” according to the New York Times. Psilocybin “has shown significant promise for treating severe depression, post-traumatic stress disorder and end-of-life anxiety among the terminally ill” — although long-term benefits remain unclear.
“All of my mom friends are microdosing mushrooms, and I want to try it, too,” a patient told Bay area psychotherapist Melissa Whippo for a Washington Post guest column. Reflecting the expanding enthusiasm for taking small doses of psilocybin, Whippo writes, “my patient lives in the Bay Area — home to one of the epicenters of what is known as the “psychedelic renaissance,” making it more common for moms to discuss microdosing at play dates.”
Meanwhile, some states and cities are moving to loosen legal restrictions on psychedelics. On January 1, Oregon began allowing anyone age 21 and older to “legally access psilocybin services”—although only under the supervision of a state-certified facilitator. The dozens of facilitators currently in training should be ready “sometime later in 2023,” according to Smithsonian magazine.
Colorado, too, has legalized supervised psilocybin use at state-approved centers, which should become available in 2024, while individuals age 21 and up will be able to use, grow and share mushrooms. Neither Colorado nor Oregon allows retail sales of the drugs. Washington D.C. and specific cities in Michigan, California, Massachusetts and Washington State have also decriminalized possession of select psychedelics.
The Pollan site lists a wide variety of psychedelic service providers—including individual “trip sitters” at sites like Psychedelic Passage, who guide personal experiences without supplying the drug. In addition to Atman, several U.S.-based organizations offer psilocybin retreats in the Bahamas, the British Virgin Islands and other countries where the drug is legal.
Another way to experience psychedelic drugs in the U.S. is to participate in research—made possible because of the FDA’s 2018 designation of psilocybin and MDMA (Ecstasy) as “breakthrough therapies” for the treatment of PTSD and depression. Ongoing trials with the Department of Veterans Affairs and at academic research centers, notably the Johns Hopkins Center for Psychedelic and Consciousness Research, generally accept specific groups of people, such as those coping with addiction and terminal cancer, as well as those suffering with PTSD and severe depression.
But outside of research programs, psychedelic experiences can be expensive. The current protocol for MDMA-assisted psychotherapy, for example, includes 42 therapy hours over 12 weeks, with one overnight stay—that could cost $13,000 to $15,000 per treatment. For psilocybin, the Hopkins research protocol calls for about 30 therapy hours, which includes two therapists for lengthy pre- and post-trip sessions, in addition to the eight or so hours of the trip experience.
“The biggest tensions [in efforts to legalize psilocybin have] erupted over the issue of affordability. Psilocybin sessions will not be covered by insurance as long as the federal government lists the drug as a Schedule 1 substance—meaning “no currently accepted medical use,” according to the New York Times.
Of organizations currently offering psilocybin experiences outside the U.S., Atman charges $2,450 for its four-day Jamaica retreats. For Oregon-based Silo Wellness, five-day Jamaican retreats “include 2 separate dosing sessions with reflection time between” at a cost of $4,595 for single occupancy and $3750 for double.
Taking psilocybin at a retreat setting with trustworthy guides makes it possible for some people to consume greater quantities of psilocybin than those who try the drug on their own or with an online guide. While hallucination images can be vivid at any dose, participants taking higher doses seem more likely to report encounters with people—from their past, their present lives and even after death.
For L.M., having his children come to him was “very meaningful,” he said. He talked about having “many conversations, speaking my mind to them.” He felt himself “reaching out” and describes “overwhelming feelings of love toward his kids and other people.” After the experience, L.M. felt “more stillness” in his daily meditations, which became “deeper and more satisfying;” and his prayer life became “enriched.” In the future, he would like to go to Atman or another psychedelic retreat once a year.
An obstacle for some people, however, is the requirement by many retreat organizations that participants stop taking other medications, such as antidepressants. Because both SSRI antidepressants and psychedelics operate on serotonin receptors, experts worry that the combination could cause excess serotonin in the brain, although some researchers have found no such interaction of the two drugs. Others suggest that those taking SSRIs long term need up to 50% more psilocybin to have the same effect.
Stopping antidepressants may be one reason I don’t try a psilocybin retreat. Also, I generally avoid group experiences, and found debriefing sessions at a 50-or so- participant retreat for holotropic breathing to be long and grueling. The Atman maximum of 12 sounds more promising.
Maybe more important, though, the low doses of psilocybin I have tried have gotten me to feel slightly more open to different experiences—even those that previously sounded unappealing. I found L.M.’s account of his Atman experience both intriguing and compelling.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
Bruce Willis’s recent diagnosis of frontotemporal dementia or degeneration (FTD) inspired Well-Being editor Mary Carpenter to update her 2018 story—along with recent research that should improve the accuracy of FTD detection, which has been fraught with high rates of false positive diagnoses.
FTD is the most common form of dementia in people under age 65 – beginning at an average age of 58. Explains medical journalist Michele Berman, the behavioral variant of FTD causes changes in personality and behavior—with nerve cell loss “in areas of the brain that control conduct, judgement, empathy, and foresight.”
Diminishing remorse was the almost-imperceptible sign to others after Virginia historian G.E. received a diagnosis of FTD. But for New Jersey filmmaker M.T., it was the room full of unopened boxes after she kept repurchasing the same expensive electronic devices. And M.T.’s most debilitating symptom, “hyperorality,” has caused her to devour inedible objects—sand and dirt, as happens with the condition called pica—along with any food in sight; and to chew on her lips and fingers.
But false positive diagnoses —when in fact FTD is not the reason for symptoms—can cause serious problems. In the case of DC-area nurse P.L., her relatives staged a legal takeover of guardianship based on her erratic behavior, which came in the wake of a tragic loss and was only temporary. Losing financial control, however, meant she was unable to pay for transportation to her work as a nurse and lost several jobs as a result; and her fight to regain independence was long and hard.
Reducing false-positive diagnoses from a high rate of 50% to 69% down to less than 10% was the major accomplishment of a recent multi-center study led by Columbia University neuropsychologist Megan Barker. What makes FTD diagnoses susceptible to error is the inability to examine brain cells directly—and brain imaging is rarely able to detect these problems. False positive diagnoses have occurred most often in younger patients, who usually turned out to be suffering from depression or alcohol abuse.
The seven core features of the condition illuminated by the new study vary depending on where cell degeneration is most prominent —in the frontal and temporal lobes, two of four lobes of the brain that work together. So-called “executive functions”—planning, motivation, inhibition, emotions, and creativity—are mostly controlled by the frontal lobe; while the temporal lobe helps coordinate memory, learning and attention, as well as regulating anxiety levels, appetite and emotion.
Apathy and behavioral disinhibition are the most common and familiar of the seven FTD features, with changes that can at first be small and limited. “Apathy tends to look like the following,” according to the Cleveland Clinic: “loss of motivation, social isolation, decline in self-care and hygiene, compulsive behaviors.”
With disinhibition, sufferers lack self-control and can become rude and self-centered. A dental patient, for example, at the first twinge of pain might slug the dentist—the result of deterioration in the part of the brain that would ordinarily inhibit such a reaction, based on the patient’s knowledge that dental treatment is necessary.
Five features, after apathy and disinhibition, identified by the new study, include irritability/agitation; reduced empathy (sometimes seen as lack of remorse); repetitive behaviors (such as hand clapping); joviality/gregariousness; and appetite changes/orality. A complicating FTD symptom is anosognosia, lack of insight that involves an inability to recognize one’s own symptoms or medical condition, including FTD.
Genetic inheritance plays a role in FTD, with some 30% of cases arising in people with a family history of FTD: having a parent with the mutated gene gives a child a 50% chance of inheriting that gene. In their “update” review, British neurology researchers explain how FTD, because it requires only one copy of a mutated gene from one parent—called an autosomal dominant pattern of inheritance—is a “highly heritable disease.”
Exposing a false positive diagnosis can depend on features of a patient’s condition that are unavailable until long after the first symptoms arise. With an average FTD life expectancy of 7-13 years, for example, an incorrect FTD diagnosis may become evident only after the individual has survived way beyond that time frame. And only a brain autopsy after death can positively identify the neurodegeneration.
Missed cases of FTD—false negatives—on the other hand, most often incorrectly receive the labels of other neurodegenerative diseases, such as Alzheimer’s, Parkinson’s or Huntington’s Disease. And progressive aphasia—the loss of ability to express or understand speech—can be, as in the case of Bruce Willis, an early symptom of FTD; or it can be the correct, final diagnosis.
“Since we announced Bruce’s diagnosis of aphasia in spring 2022, Bruce’s condition has progressed and we now have a more specific diagnosis: frontotemporal dementia (known as FTD),” according to the Willis family statement on the Association for Frontotemporal Degeneration website. “Unfortunately, challenges with communication are just one symptom of the disease Bruce faces.”
I met G.E. on a biking trip, and only once when she returned very late for the next activity were symptoms evident—and her friend told us about the FTD diagnosis. Soon afterwards and before her condition became more challenging, G.E. died in a freak accident. But M.T., a childhood friend, continues to suffer worsening symptoms in a special FTD care center, where she must be carefully watched and often restrained but still manages to harm herself. Friends and relatives of both women are grateful that diagnosis of someone well known like Bruce Willis brings greater awareness of the condition.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
TWO DRUGS—Wegovy, FDA-approved for weight loss in those who are obese or overweight with health problems; and Ozempic, FDA-approved for Type 2 diabetes—are different formulations of the same hormone-imitator semaglutide. As a result, when Wegovy supplies ran short recently due to high demand and a manufacturing snafu, people trying to lose weight turned to off-label use of Ozempic, which in turn created a shortage for those with Type 2 diabetes who depend on the drug.
“Ozempic Runs Low for Diabetes Patients as Weight-Loss Use Surges” was the headline on a “most popular” Wall Street Journal story last week. Elon Musk, celebrities and many others touting weight loss from both drugs have fueled more than 700 million views of Ozempic-related hashtags on TikTok.
While insurance covers Ozempic for patients with a Type 2 diabetes diagnosis, most insurance doesn’t cover any weight-loss drug. Patients taking either of the semaglutide drugs for weight loss must pay full price, which for a month of treatment via weekly injections, comes to about $892 for Ozempic and about $1,350 for Wegovy.
“I’m middle class and a good example of someone who needs to lose weight but cannot afford these drugs,” says local foundation executive R.D. Critics decry the failure of most health plans serving older adults and low-income families, often the people who most urgently need medical help for overweight or obesity—to cover weight loss drugs, although Medicare pays for bariatric surgery.
“These anti-obesity medications are the best we’ve ever seen,” said Tulane obesity specialist Shauna Levy. “Patients I see want their knees to feel better, their hips to feel better, their blood pressure to get better, their diabetes to get better,” Levy said. “But when they come in, I have to tell them, ‘I’m sorry, I’d prescribe this for you, but it’s going to be $1,200 a month because your insurance doesn’t cover it.’ It’s sad.”
Being overweight and having “pre-diabetes” (blood sugar levels just below those for a Type 2 diabetes diagnosis) are the top two risk factors listed by the CDC for Type 2 diabetes. In both Type 1 and Type 2, though for different reasons, insulin is no longer doing its job of processing glucose, which then circulates at high levels in the bloodstream. Persistent hyperglycemia can impair the body’s ability to fight off infections—putting diabetics at higher risk for infections in the urinary tract, lungs, skin and elsewhere—as well as damaging blood vessels throughout the body with serious health consequences.
Proponents of the semaglutide drugs’ use for weight loss emphasize the need to take them in conjunction with improving diet and regular exercise—without which beneficial effects may not endure. Likewise, among reasons given by insurers for their refusal to cover any weight-loss drug is the drugs’ failure to insure weight loss once a patient stops taking them, along with limited evidence of lasting benefits in reducing risk of diabetes or cardiovascular disease.
Serious health complications can arise for Type 2 diabetes sufferers who are unable to fill their Ozempic prescriptions. “When people suddenly stop semaglutide, the amount of glucose in their blood can surge,” as American Diabetes Association medical advisor Robert Gabby told the New York Times. “Patients with diabetes may experience blurry vision, fatigue and excessive thirst and urination…end up in the emergency room from exhaustion.”
Diabetes patients unable to locate semaglutide medication also face higher risk of heart failure, the most common cardiovascular disease in patients with Type 2 diabetes. In small studies of patients with both Type 2 diabetes and obesity, these drugs reduced ER visits and hospitalizations due to heart failure.
Semaglutide drugs work by mimicking hormones called incretins, which delay gastric emptying and activate satiety centers in the brain, creating a sensation of fullness that helps suppress appetite. At the same time, the drugs boost insulin production in the pancreas to help control blood glucose levels after eating. A newer drug, Mounjaro, employs a different chemical—tirzepatide— which also mimics incretins but acts on two different kinds of receptors, rather than just the one affected by semaglutide. Mounjaro, expected to receive FDA approval for weight loss, will cost about $975 a month.
Side effects of incretin-mimicking weight-loss drugs include feelings of nausea, vomiting, constipation and abdominal pain. Another unwanted effect is gauntness and sagging facial skin, common with weight loss for any reason but for people taking these drugs known as “Ozempic face.”
A different drug, Metformin, is often the first one prescribed for Type 2 diabetes patients but is also used off-label for weight-loss. Taken in a twice-daily pill, Metformin works by decreasing sugar absorption from the intestines, lowering the amount of glucose produced by the liver and improving insulin sensitivity. And the drug has received recent attention for its potential to stave off effects of aging —by creating greater resilience, especially against severe disease.
Plenity is an absorbent hydrogel pill available by prescription and designed solely for weight loss. Dubbed a “bloating drug,” Plenity—taken before meals with 16 ounces of water—creates feelings of fullness by decreasing the stomach’s volume by about 25%. Side effects include abdominal distension as well as bloating. In research, participants taking Plenity have lost an average 10% of body weight in six months; those taking Wegovy achieved weight loss closer to 15-20% of their body weight, which is comparable to that of bariatric surgery.
Among an array of OTC options, L-glutamine supplements work by altering composition of the gut microbiome and may improve blood sugar control. Studies on these drugs’ effects on insulin as well as their success in achieving long-term weight loss has produced unclear results. Glutamine also occurs naturally in foods, including eggs, beef and tofu.
Some people struggling to control their weight, however, are not satisfied by feelings of fullness or helped by blood sugar control—as evidenced by those who have bariatric surgery to reduce stomach size but continue to overeat despite serious health complications. In some cases, people eat compulsively for emotional reasons, for example, trying to combat depression or feelings of emptiness.
And some 13% of the over-50 population who overeat sugary or salty foods have symptoms of addiction that include intense cravings. They attempt unsuccessfully to cut back on consumption and experience symptoms of withdrawal, such as irritability and headaches.
My worst experience of gaining too much weight, about 60 pounds in a month, came during an emotional crisis that led to me dropping out of college. The foods I couldn’t stop eating, way past feelings of fullness, were mostly very sugary and salty. After about nine months, I returned to college and started losing weight—with a new understanding and sympathy for anyone who has trouble resisting such intense cravings.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
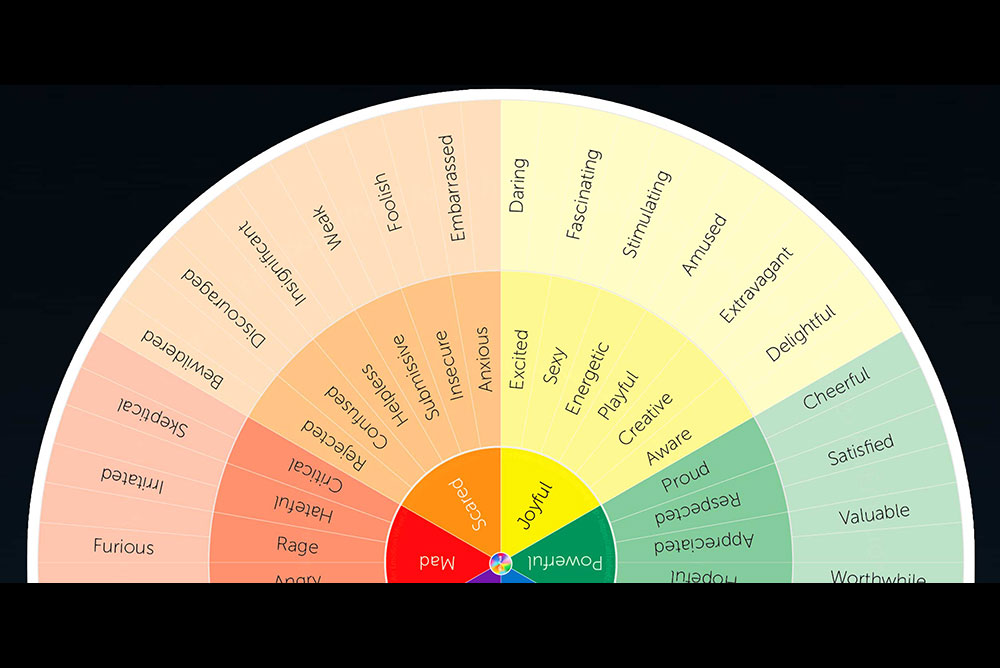




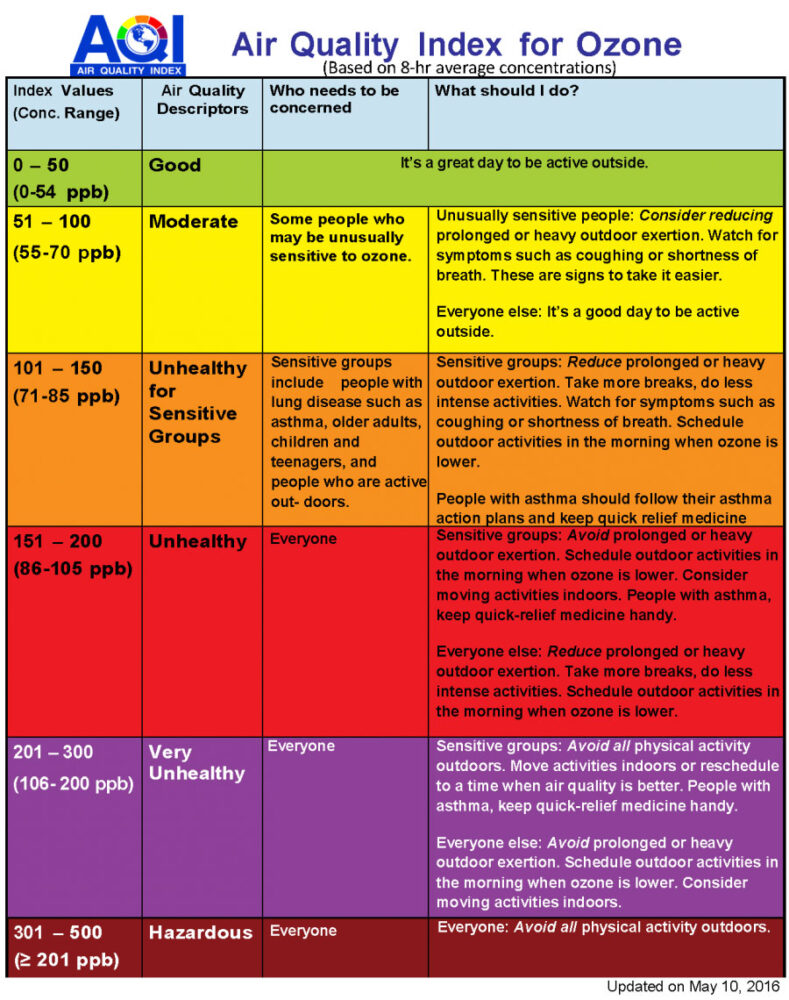
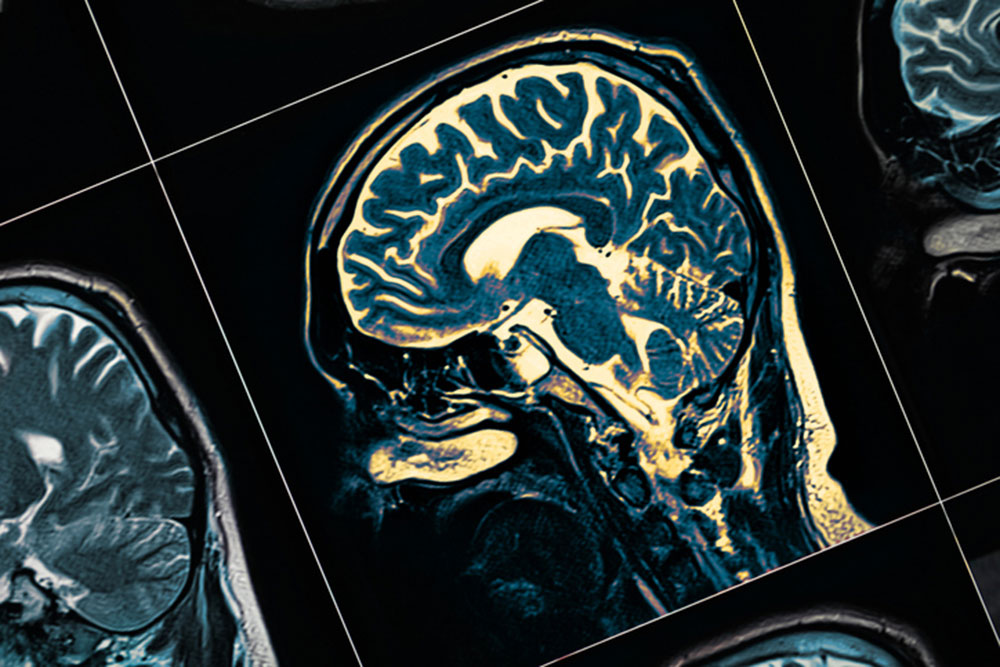


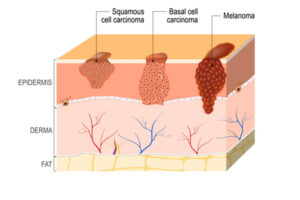
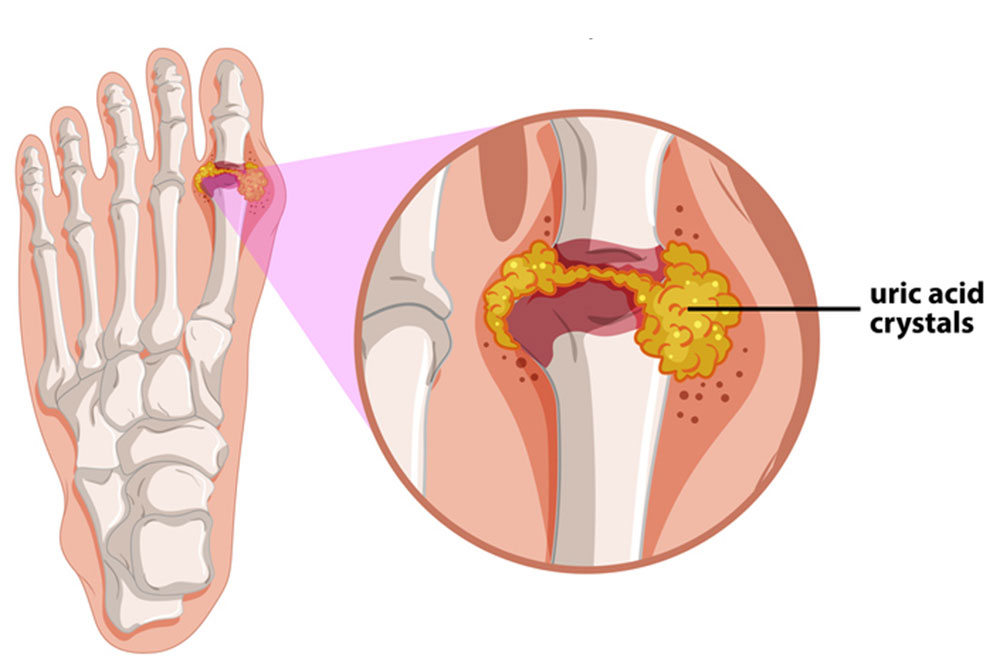




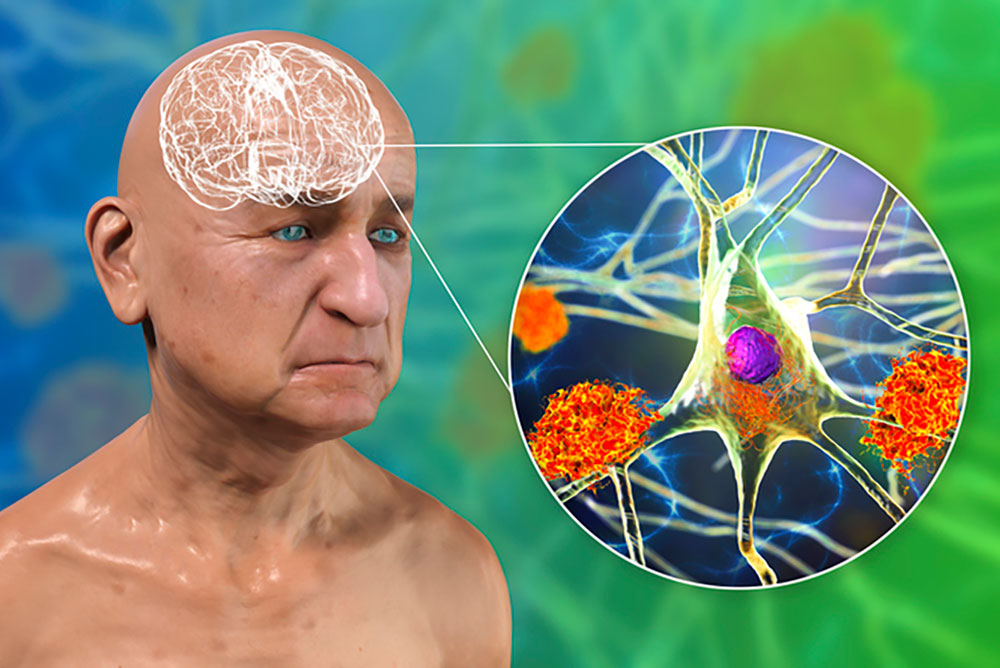


{kind=link}