JOINT dysfunction that occurs without any acute physical injury or after one has been resolved can involve two different issues. Arthritis is the most common cause of physical or structural problems, which are visible on scans and diagnosed by health practitioners.
But pain, the second kind of issue, can be difficult to trace, document and diagnose—with scans of arthritic joints often a distraction from the real cause. In the DC area, a writer’s shooting pain down one leg initially blamed on her arthritic back turned out to be coming from a torn meniscus (in the knee). For another woman, scheduled for replacement of a painful arthritic hip, the problem was a small piece of spinal cartilage pressing on a nerve. She needed a simple cortisone shot to dissolve it.
Chronic pain poses the greatest conundrums, with several factors contributing to the establishment of neural pathways that cause pain to persist. “Approximately 85% of back pain and 78% of headaches don’t have an identifiable trigger,” according to Dartmouth neuroscientist Tor Wager. Instead, circuitry malfunctions in the brain can prolong, amplify and even create pain— the result of ongoing stressors, known to promote inflammation in the spinal cord and brain; or to early adversity, such as child abuse and neglect.
Discovery of this “phenomenon of central sensitization” in the early 1980s led to the understanding that pain is not always a symptom reflecting a disease but “often is a consequence of a disease state of the nervous system itself,” Harvard neurobiologist Clifford Woolf told the New York Times. The pain of fibromyalgia, for example, does not emanate from a single problem but occurs throughout the body and may be, Woolf said, “solely a problem of the central nervous system.”
Determining the best treatment for an individual’s joint dysfunction can be difficult when structural symptoms and pain exist together as occurs in osteoarthritis (OA). According to WebMD, “Using your joints over and over damages the cartilage, leading to pain and swelling. Water builds up in the cartilage, and its proteins break down…in severe cases you can lose all the cartilage between the bones of a joint.”
“The fundamental problem of osteoarthritis is thought to be the imbalance between natural degradation [the joint surface wearing away with use] and fresh cartilage production,” according to verywellhealth. The body’s inability to compensate for lost cartilage “is partly normal wear and tear and partly disease process,” which can cause damage to the bone as well as inflammation of the soft tissues.
Where doctors often disagree is for patients whose scans show joints riddled with arthritis or without any cartilage left, but they experience little or no pain. Looking at the disconnect between pain and progression of osteoporosis, researchers in Boston and Korea described reports that, “knee pain is a better predictor of disability than radiographic changes.”
Among drawbacks weighed against the benefits of joint replacement is the risk of chronic postsurgical pain. In a British study of 34 people, postsurgical discomfort included “heaviness, numbness, pressure and tightness associated with the prosthesis.” In addition, infection occurs in about 1% of patients following joint replacement surgery.
But worries about a lengthy rehab is the main reason many hesitate to have joints replaced. For knee replacement, “average recovery time is approximately six months…it can take roughly 12 months to fully return to physically demanding activities,” according to Tri-State Orthopedics. If the joint is not replaced, on the other hand, physical impairments with or without pain can cause instability and structural changes in posture or lead to the need for replacement at an older age when surgery poses additional challenges.
Body weight is another source of disagreement, along with the usefulness of BMI measurements. Following orthopedists’ advice to lose weight has, for some patients, led to joint pain improving or disappearing entirely. And some orthopedists require patients to lose weight before joint replacement, citing evidence that patients with a BMI above 40 are more likely to experience serious complications during and after surgery.
Replacing the painful joint for patients with high BMI scores, however, can enable them to exercise more and lead to better overall health. And BMI scores are not always good predictors of surgical outcomes because they don’t account for variables such as fitness, genetics and pre-existing conditions.
Many patients with joint complaints choose to tackle pain symptoms before deciding about surgery. One option is a course of NSAIDS: for example, taking a “medical dose” of Alleve (two 220 mg. pills) morning and night for four or five days, with analgesic effects building up over time. Another drug option, cortisone shots, can both reduce inflammation and dissolve problematic tissue.
Electrical stimulation of nerves or muscles offers a different approach to chronic pain. Transcutaneous Electrical Nerve Stimulation (TENS) employs electrodes attached to the skin that send an electric current to the nerves—which in turn overrides pain signals from the brain. The current may also trigger the release from the brain of endorphins that are considered “natural pain killers.”
Neuromuscular Electrical Stimulation (NMES) involves electrical impulses strong enough to make the muscles contract—which, combined with an exercise program, can strengthen muscles that support weakened joints. In a 12-week home exercise program for knees, NMES reduced pain in 64% of patients compared to 42% in the control group who received sham (placebo) treatment—and improved strength and stability in the knees.
Engaging the brain is a different route to pain reduction—in line with the concept of central sensitization that pain is a “brain response [to perceived danger] like…elevated heart rate,” writes Cornell University researcher Nathaniel Frank in the Washington Post. In research on 151 patients at the University of Colorado at Boulder, the group of patients receiving eight one-hour sessions of “pain reprocessing therapy” (PRT) learned to “reinterpret pain as a neutral sensation coming from the brain.
Teaching PRT patients that their pain might be uncomfortable—but did not signal a dangerous physical condition—led their brains to rewire those neural pathways that were generating pain signals, Frank explained. Of patients receiving PRT, 66% were nearly pain-free and 98% had some improvement. In a separate study on psychophysiologic symptom relief therapy by Harvard researchers, mind-body therapy courses that focused on pain were significantly more effective than other mindfulness and stress-reduction programs.
For me, most joints are “full of arthritis,” as one orthopedist put it—neck, shoulder, back, hip and knee—but rarely painful. When I once mentioned occasional pain if standing with a bent knee in yoga class, the orthopedist’s response was a resounding, “You must never do yoga!” But several others, using the same wording, said that in the absence of pain, I “might not be happy” with new joints.
Other issues with my knees and hips, such as instability, may at some point convince me to have replacements. Meanwhile, I wear protective bands and braces, occasionally take a short course of strong NSAIDS and am otherwise engaged in a lifelong quest for stress reduction and mindfulness—with the idea that these could at least keep instability from doing me in.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
THE RECENT proposal to put Covid vaccinations on a regular annual schedule has raised new questions—specifically about the future of Covid vaccines but also about vaccinations in general. While repeat Covid vaccines without a sufficient several-month interval between shots could reduce the impact of each shot, all currently recommended vaccines not only confer disease protection but might also be good for brain health.
“All types of vaccinations were associated with a trend toward reduced dementia risk,” according to a multicenter study by Chinese researchers. Comparing dementia risk in vaccinated versus unvaccinated populations in 17 studies (altogether 1,857,134 participants), their analysis found vaccinations associated with a 35% lower dementia risk.
“Routine adult vaccination… may be an effective strategy for dementia prevention,” write the Chinese researchers. “A growing body of research suggests that the immune system and infections play an important role in the development of dementia: bacterial, fungal and viral infections may cause neurotoxic inflammation and oxidative stress in the brain, which can lead to neurodegeneration.”
“People who received at least one influenza vaccine were 40% less likely than their non-vaccinated peers to develop Alzheimer’s disease over the course of four years,” report neurologists Avram Bukhbinder, now at Mass General, and Paul Schultz at University of Texas, Houston—who looked at the effects of flu vaccination on a large nationwide sample of adults age 65 and older. “The strength of this protective effect increased with the number of years that a person received an annual flu vaccine.”
“Vaccinations against flu, pneumonia and shingles appear to offer protection against Alzheimer’s and Parkinson’s diseases, the most frequent forms of age-related neurodegeneration,” according to radiation oncologist Steven Lehrer at Mt. Sinai in New York. Other vaccines associated with “significant” reduced dementia risk by the Chinese researchers: rabies, tdap (tetanus, diphtheria and pertussis) and hepatitis B.
Vaccines may help reduce the risk of dementia by preventing infectious diseases that create system-wide inflammation. But that can’t be the whole story, because while different vaccines have varying efficacies against the relevant pathogens, Lehrer writes, “significant reductions in dementia risk can be observed after almost all types of vaccination.”
“Protection against bacterial and viral infection is beneficial to the brain since these infections may activate dormant herpes simplex type 1 and herpes zoster virus,” he suggests. Another theory involves off-target or non-specific effects (NSEs) of vaccinations, for example, training the body’s immune system to prevent pathogens from entering the brain and thus reducing the risk of dementia caused by chronic and abnormal neuroinflammation.
One “unanswered question: are the AD-risk-reducing effects of flu, pneumonia, and shingles vaccinations cumulative?” asks Lehrer. And one caveat noted by the Chinese researchers: Although most vaccine studies control for demographics, comorbidities and medication use, the brain-protection effect of vaccination might reflect “the different health characteristics and lifestyles between vaccinated and unvaccinated populations, such as better knowledge of disease prevention, higher education and income, and greater social support.”
The only seasonal vaccine currently recommended by the CDC is for influenza. In addition, adults 50 and older should receive the shingles vaccine, and those 65 and older should get vaccine protection against pneumonia. Adults who did not receive the pertussis vaccine as an adolescent should receive one Tdap vaccine, and all adults should get Td (tetanus and diphtheria) or Tdap every ten years.
For chickenpox, likely exposure to the virus for anyone born before approval of the varicella vaccine in 1995 should provide immunity. And the recommendation for vaccination against hepatitis B covers ages 19 through 59, as well as those 60 and older with risk factors or who choose to get the vaccine.
For the proposed annual Covid vaccination, too many questions about the virus remain unanswered, according to the NBC report on the FDA advisory committee’s review. Because Covid has failed to settle into a predictable seasonal pattern like that of the flu, for example, it could be hard to determine when to schedule such a vaccine. Said New England Journal of Medicine Editor-in-Chief Eric Rubin, “The virus may mutate multiple times a year or it may not.”
Boosting every six months provided “very strong suppression” of infection, according to an analysis by researchers at the University of North Carolina at Charlotte and Yale University. In their six-year projection, one in 10 people who received updated boosters every six months would contract Covid —compared to three out of 10 of those who received an annual shot, and nine out of 10 among those who didn’t get a booster at all.
“The durability question “is a big one,” University of Toronto immunologist Jennifer Gommerman told Science —whether an annual Covid booster could offer enough protection for a whole year, and how much that might vary by a person’s age. Experts worry that policy decisions might outpace the data.
For now, confusion over how well boosters work may be one reason for low uptake of the newer bivalent shot—by only 40% of people 65 and older, the most vulnerable population. Many mistakenly believe they are protected against infection or severe disease because of previous vaccination or infection, while others appear wary of the new-technology messenger-RNA vaccines made by Pfizer and Moderna—or are reluctant to undergo the side effects, such as flu-like symptoms that can persist for several days.
The bivalent booster has, in new research from this January, proved as effective against the latest Omicron viral sub-variants XBB and XBB.1.5 as it was against earlier sub-variants. Based on North Carolina vaccine registry data for those over age 12, the booster showed 58.7% effectiveness against hospitalization compared to 25% for the original monovalent vaccine, as well as 61.8% effectiveness against infection versus 24.9% for the earlier vaccine.
But this research shows effectiveness only “for at least the first three months after vaccination,” as does most other Covid vaccine research. I’ve had two bivalent boosters, the last one five months ago, and am having trouble finding out whether and how to get what would be my sixth Covid vaccine. With new information about how vaccination might boost brain health, I’m ready for my next shot.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
LOCAL nonprofit founder L.D., who swims and walks regularly, spent a morning shivering on the couch. Trying to take a shower, she became so dizzy she crawled out on her hands and knees. As the day progressed, she began shaking uncontrollably and felt cold under heavy blankets as her fever rose to 102. At the hospital on her doctor’s advice, ER physicians diagnosed sepsis, transferred her to an in-patient bed and started IV antibiotic treatment.
The Covid pandemic has shined new light on sepsis because of overlapping symptoms, including those experienced by L.D. Also, the two conditions operate via common mechanisms: overreaction of the immune system to infection leading to system-wide inflammation, called a “cytokine storm.” In addition, Covid infection can make sufferers more susceptible to other infections, making diagnosis and treatment more complicated.
“Whenever the immune system is highjacked by a microbe, the body’s defenses can become self-destructive,” explains New Jersey surgeon Richard Marfuggi and colleagues on STAT. “The pathogens shut down one part of the immune cascade while shifting another part into a hyperactive state.” The result is the creation of micro-clots capable of cutting off blood supply to the organs and causing them to fail.
Rapid treatment of sepsis is important: Every hour delay increases the “odds of a poor outcome by 3 to 7%,” according to STAT. But difficulty pinning down the cause and location of the infection can make sepsis tricky to treat. In most cases, the villains are bacteria—in the lungs (pneumonia), the urinary tract (UTIs) and abdomen (appendicitis)—and will respond to antibiotics. But other infectious agents, such as the virus causing Covid, require different kinds of drugs.
Sepsis kills about 350,000 Americans each year, including up to 40% of those who develop severe sepsis and septic shock, making it the most expensive in-patient therapeutic cost and the most costly in-patient condition covered by Medicare. More than 80% of people in one survey were unfamiliar with its symptoms—compared to recognizing signs of stroke (facial droop and slurred speech) and heart attack (chest and left arm pain)—as well as with the acronyms designed to help recognize sepsis.
The acronym TIME refers to “temperature, infection, mental decline and extremely ill,” according to PennMedicine. And “SEPSIS denotes shivering, extreme pain, pale skin, sleepiness, I feel like I might die, and shortness of breath.”
“Apart from a few major academic medical centers, most patients and clinicians lack access to the latest diagnostic technologies,” according to the STAT editorial. The result can be “disease progression that makes patients sicker, more likely to need hospitalization and more difficult to cure.”
In L.D.’s case, her original infection was a UTI, and her ER diagnosis was pyelonephritis—inflammation of the kidney due to bacterial infection. According to UrologyHealth, E.coli and other bacteria that live in the intestines can travel upwards into the urinary tract via the urethra and on up into the bladder, causing either cystitis (inflammation of the bladder) or a UTI. From there, bacteria can proceed up the ureter into the kidneys.
“The body often can fight off simple UTIs on its own,” according to Medstar Health. AZO, the OTC pain reliever phenazopyridine, deals with symptoms of pain, burning, increased urination and the increased urge to urinate, but doesn’t treat the infection. Prescribing antibiotics for a potential UTI usually depends on the presence of multiple symptoms, such as fever or burning sensation while urinating.
About 1 in every 30 cases of UTI leads to a potentially dangerous kidney infection, more commonly in women who have frequent bladder infections or anything that blocks urine flow, such as kidney stones and structural problem in the urinary tract. Also, UTIs occur more often in postmenopausal women, whose bodies produce less estrogen, making the urinary tract more susceptible to bacterial growth. “Treatment bundles” for sepsis include medication to treat the infection and infused fluids to encourage blood circulation and recovery.
As sepsis continues to deserve better attention, the Covid pandemic may be waning. In last week’s New York Times final “Virus Briefing” email, which began March 2, 2020, science reporter Carl Zimmer wrote: “Nearly 4,000 Americans died just last week of Covid-19—from a disease that did not exist four years ago. Sixty-five million people are estimated to have long Covid…SARS-CoV-2 is continuing to evolve in surprising ways. This story is not over.” National reporter Mitch Smith writes, “I’m struck by how far we have come and how far we have not. Covid, rather than becoming a past-tense plague, has remained a present-tense threat, even if it’s less of one before…”
Deaths from Covid now amount to around 180,000 a year, still a much higher number than the 12,000 to 52,000 annual deaths associated with flu. These totals, however, remain much lower than than the 350,000 each year linked to sepsis.
And even when sepsis is not the diagnosis, symptoms such as shivering and feeling clammy can signal serious infection: a friend with these symptoms recently needed immediate treatment for pneumonia. But for the only other person I know who developed sepsis, early 50s DC-based filmmaker L.K., the original infection came from a cut on her toe. Because I have peripheral neuropathy that causes diminished feeling in my feet, I watch out, take care and see a doctor when I’m worried.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
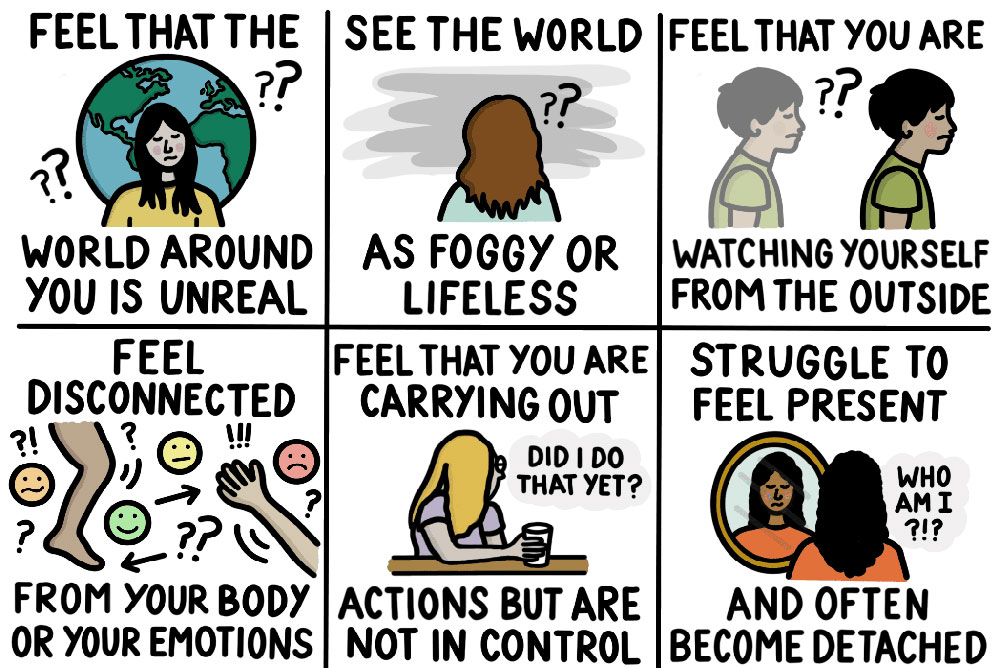
MILD concussion, frequent fainting, long-haul Covid and even jet lag—all share physical sensations of being out of whack, out of sync, that fall under the increasingly familiar label dysautonomia. The nonprofit Dysautonomia Project’s seven-item “symptom checker” list includes brain fog, fatigue, lightheadedness, shortness of breath, GI symptoms, chest discomfort and difficulty standing still.
Vasovagal syncope—also called the simple faint, and a common sign of dysautonomia— seemed the obvious diagnosis for Maureen Ryan, subject of a recent Washington Post “medical mystery.” Although Ryan had fainted often over many years, when she woke up in a Seattle park after a solo run feeling terrified and vulnerable, she decided to seek medical help.
“Someone is considered to have syncope if they become unconscious and go limp, then soon recover,” according to the Johns Hopkins site. Vasovagal refers to a temporary fall in blood pressure caused by overactivity of the vagus nerve, the long wandering nerve that connects the body and the brain. In vasovagal syncope, the most common form of reflex syncope, the heart slows or the blood vessels dilate as a reflex response to a trigger—often a combination of dehydration and upright posture as in prolonged exercise, or emotional as in “fainting at the sight of blood” (or a needle).
Dysautonomia also underlies the diagnosis of POTS (postural orthostatic tachycardia syndrome) or lightheadedness on standing up. If blood remains in the lower part of the body, the heart beats faster and blood pressure drops suddenly—often occurring in the wake of an infection when auto-immune markers remain in the blood.
But the immediate cause is the body’s failure to react—to get blood moving back up toward the head—via the autonomic nervous system (ANS), which is responsible for maintaining equilibrium or homeostasis in the body. According to Mayo Clinic neurologist Jeremy Cutsforth-Gregory, “Dysautonomia is probably significantly more common than we realize…it’s significantly underdiagnosed.”
What can be out of whack comes from imbalance between the autonomic nervous system’s two branches — the sympathetic and parasympathetic nervous systems (SNS and PNS). With an overactive SNS and underactive PNS—called sympathetic dominance —the release of hormones such as adrenaline, usually involved in a sudden but brief fight-or-flight response, can persist over time. A healthy parasympathetic nervous system, on the other hand, counters the stress response by lowering heart rate and blood pressure.
Even mild concussion—including one caused by a hit with a dog toy—can keep the two systems out of balance. The nervous system’s connection to the body through a cluster of cranial nerves at the base of the skull makes it vulnerable to injury from outside forces. After D.C. artist and teacher A.M. hit her head on a pole rushing to get off a Metro train, symptoms began with headaches and facial pain focused in her jaw, but what caused the most trouble was extreme sensitivity of her eyes to any light, indoors and outside, that lasted for months.
When patients with long Covid listed lightheadedness, brain fog and fatigue among their symptoms, doctors began testing for dysautonomia. Finding indicators in almost two-thirds of patients led to speculation about a lasting autoimmune reaction to the virus.
And interference with sleep cycles due either to sleep restriction or to misalignment of sleep times with circadian rhythms—the desynchrony that occurs with jet lag—has led to “impaired autonomic function,” according to researchers at the University of Chicago investigating the effects of these on blood pressure and cardiovascular risk.
The heart also offers the best means of assessing dysautonomia, specifically heart rate variability (HRA). A Holter monitor, a noninvasive device with electrodes attached to the chest, can record variations in heart rate over 24 hours —with greater variability, sometimes elevated and sometimes low, indicating a healthier autonomic nervous system. Dysautonomia treatment focuses on individual symptoms: for blood pressure, using medication; or in the case of low blood pressure, making lifestyle changes such as adding salt and drinking more liquids.
Drinking liquids is also the best immediate recourse for feeling faint—along with raising the legs higher than the head to help get the blood flowing in the right direction. Other possibilities involve working directly on the vagus nerve to spur activity in the parasympathetic nervous system by way of the vocal cords—with activities that include gargling, singing and humming. When yoga teachers encourage the chanting of ohm, extending the sound deep into the throat can produce a sort of vibration that can help with moving from hectic daily life to focused poses of yoga.
But dysautonomia can also be a misleading default diagnosis. In Maureen Ryan’s medical mystery, vasovagal syncope was incorrect—because “at the peak of exercise the vagal response does not kick in,” according to cardiologist and electrophysiologist Samir Saba at the University of Pittsburgh Medical Center. Instead, the problem turned out to be an anomalous right coronary artery originating from the wrong location, detected by MRI, that caused “severe compression [limiting] blood flow at the peak of exertion.”
While excess summer heat or sun exposure can make me feel faint, cramping is my earliest sign of trouble. What has helped is “Saltstick Fastchews,” which taste something like sweet tarts and include small amounts of four electrolytes. I started eating one every now and then in warm weather and now take one most every day—maybe too little to make a real difference, but something easy I can do that seems to help.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
MyLittleBird often includes links to products we write about. Our editorial choices are made independently; nonetheless, a purchase made through such a link can sometimes result in MyLittleBird receiving a commission on the sale. We are also an Amazon Associate.
DIFFERENCES in individuals’ microbiomes can alter, sometimes dangerously, the effects of prescription drugs—from antibiotics and antipsychotics to the diabetes drug metformin and the statin rosuvastatin. Of 1,000 drugs screened in a 2018 study, nearly one-quarter had antibiotic effects, though none were being sold as antibiotics. (The microbiome refers to bacteria populating an individual’s gut—which antibiotics can alter, sometimes dramatically.)
“It was possible to essentially transplant a mood disorder into rats,” Nature writer Neil Savage reports on studies at APC Microbiome Ireland. Led by psychiatrist Ted Dinan, the researchers first wiped out rats’ native microbes using antibiotics and then gave them a “dose of gut bacteria” from people being treated for depression—with the result that their behavior was “significantly altered.”
Pharmaceuticals and bacteria have an undeniable effect on each other,” writes Savage. Dinan deems the gut microbiome a “virtual organ in its own right,” and predicts that “in a few years [the US Food and Drug Administration will not] license any drug unless its impact on that virtual organ has been studied.”
More than 200 drugs, prescribed to more than one-third of U.S. adults, have depression or suicide listed as potential side effects on accompanying labels—but in fine print and often unread according to 2018 data from the multi-year NHANES (National Health and Nutrition Examination Survey) study with more than 25,000 participants. About 5% of people taking drugs on the list —including heart and blood pressure medicine and antacids—experienced depression; and of those taking two of the drugs at the same time, 9% became depressed.
“No one knows exactly why certain drugs have this effect,” according to the Health.com report on the NHANES study.University of Miami Clinical Psychiatry Professor Edmi Cortes Torres suggested that “the medications may interfere with neurotransmitters…like dopamine and serotonin.”
The ability of certain “good” bacteria to synthesize neurotransmitters, as well as those chemicals the body uses to produce mood-regulators such as serotonin, may explain the link between low diversity of gut microbes and mental health conditions such as schizophrenia. In addition, with psychotropic drugs, such as those used in treating Parkinson’s disease, gut molecules that break down the drug can significantly decrease the amount that reaches the brain.
Notable for its varying effect on different individuals, the drug rosuvastatin in a 2016 study produced a 50% drop in LDL cholesterol in 46% of patients, but 11% of participants had no reduction or even had an increase in LDL. Psychopharmacogeneticist Sony Tuteja at the University of Pennsylvania suggests that the drug might throw microbes in the intestinal tract out of balance in a way that either alters cholesterol metabolism or that renders the statins less effective.
“It could be bidirectional,” says Tuteja. “The microbiome is affecting the drug and the drug is affecting the microbiome.” Savage explains the possibility that using statins to lower LDL levels can make the gut “more congenial for some bacteria and less so for others.”
The antibiotics Cipro and Levaquin, in the drug class fluoroquinolones, have since 2018 carried the FDA’s strongest “black box” warning. The warning associates these drugs with “disabling and potentially permanent” side effects on the central nervous system, nerves, muscles and joints—which include causing Achilles tendon tears. According to the FDA, the benefit of taking these drugs may not be worth the risk.
The CDC has denied a petition from South Carolina oncologist and public safety expert Charles Bennett asking that suicide be added to the black box warning on fluoroquinolones, but it may accede to Bennett’s request that “long-term toxicity” caused by the drugs be recognized as a condition covered by insurance.
The penicillin-based antibiotic Amoxicillin carries warnings for sedation, anxiety and hallucinations, and has been linked to three reported cases of psychosis. And doxycycline, along with other tetracycline antibiotics, risks causing sexual dysfunction—indicating the possibility that it inhibits serotonin reuptake, which could explain its risk for suicide.
Besides implications for drug treatment, microbiome differences can affect the success of fecal transplantation, a medical approach to persistent infection with the bacterium C.diff., which can be severe and even fatal. Because previous antibiotic treatment of C.diff. may have altered the balance of healthy bacteria in the gut, fecal transplants administered via colonoscopy or using upper endoscopy can restore a healthy balance.
Fecal transplants may also help with symptoms of Irritable Bowel Syndrome (IBS), a condition with no clear cause but linked to unhealthy microbiota. In a 2018 Norwegian study of 164 IBS patients, depending on the dose, 75% and 89% of those receiving fecal transplantation showed improvement that was sustained for at least a year—although 23.6% in the placebo group also reported improved symptoms. According to NBC, the study used transplant samples from a so-called “super donor [who had been] breast fed, consumed a nutritious diet, took no regular medications, was a nonsmoker and had taken antibiotics only a few times.”
Among seven large studies using fecal transplantation for IBS symptoms included in a 2021 survey, however, positive effects occurred in only four—with no effect in the other three studies. But the survey also revealed “marked differences” among the studies on a number of variables, including selection processes for the donors and patients, transplant dose and route of administration.
The constantly changing makeup of an individual’s microbiome may pose difficulties in treatment approaches. Developers working on algorithms for microbiome-based diet apps, for example—which recommend food choices based on an individual’s microbiome—rely on genetic profile and family history but must also respond to fluctuating factors such as physical activity, sleep, stress and medications.
Three of my close family members, unrelated to each other, suffered torn Achilles tendons while taking Cipro. And while for the past six months I expected rosuvastatin was making it okay to consume cholesterol with abandon, I now know the drug could be having no effect or even increasing my LDL levels. I also just learned that eating foods high in fat or cholesterol can reduce its effectiveness.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
A TWENTY-SOMETHING athlete fell to the ground recently at a DC-area gym, telling those nearby he had asthma and couldn’t breathe. No one called 911 —because most listings of emergencies requiring immediate treatment do not mention asthma and because most people underestimate its dangers. While his worried friend was rushing to purchase an inhaler, the boy died.
Most published emergency lists are predictable, with heart attack usually at the top. Warning signs are familiar. For heart attack, one list includes “pale skin, a cold sweat, exhaustion, a tightening of the back and chest…and pain that radiates from the chest to the arms, shoulders, and neck.” Following heart attack, this list prioritizes choking, car accident, fire and profuse bleeding.
Such familiar heart attack signs, on the other hand, don’t always apply to women—who are “much more likely to get…indigestion, shortness of breath and back pain, sometimes even in the absence of obvious chest discomfort,” according to Johns Hopkins Heart Failure Clinic director Lili Barouch.
Stroke on these lists only appears first under headache, at #15;” followed by #16, “stroke symptoms”—although in the stroke-warning acronym FAST, the “T” points to the crucial element of time elapsing before treatment to achieve the best outcome. For the other three letters, symptoms that necessitate emergency care include F for drooping face (check the smile); A for arm weakness (raise both arms and compare); and S for speech difficulty (repeat a simple sentence like “the sky is blue”).
Heart disease remains the country’s number one killer. In 2021 updated statistics, CVD (cardiovascular disease) is responsible for 2,380 deaths per day—and 12% of people having a heart attack will die from it. Stroke accounts for 405 deaths every day.
Asthma, meanwhile, kills about 11 Americans each day, although some 25 million people in the U.S — one in 13 —live with the condition. Female adults are more likely to have asthma and to die from it than male adults. According to the Asthma and Allergy Foundation of America, “nearly all of these [asthma] deaths are avoidable with the right treatment and care.”
The symptoms of chest discomfort or pain that signal asthma, however, can be very similar to those of a heart attack. Pediatrics professor at Minnesota’s Mayo Clinic Young Juhn stresses the importance of differentiating the two problems “because asthma increases the risk of heart attack and treatments for each are quite different.”
“Asthma attacks tend to sneak up [on the sufferer] before you notice symptoms have worsened,” according to the Mayo Clinic. One clue that someone might be having a serious attack is the “inability to speak more than short phrases due to shortness of breath.” Others include severe breathlessness or wheezing and having to strain chest muscles in order to breathe.
“It feels like an elephant is sitting on your chest,” said local filmmaker L.K., a family friend of the boy who died recently and who always carries with her the prescription “rescue” inhaler albuterol. (“Rescue” or “reliever” inhalers differ from “preventer” options that include different inhalers as well as long-acting bronchodilators.) L.K. traces her asthma to early childhood years spent with parents who smoked several packs of cigarettes a day.
Usually beginning in childhood, asthma narrows the airways and produces excess mucus—and can result from the environment, such as with family members who smoke as well as from inherited genes and from having respiratory infections during infancy or childhood. But it can also arise in adults, linked to smoking, obesity and female hormones. Of three telltale asthma symptoms, the “classic” one is wheezing, a high-pitched whistling sound created by obstructed bronchial passages, along with shortness of breath and cough.
Like asthma, bronchitis can also involve wheezing and shortness of breath, but the main symptom of “acute” bronchitis is a cough lasting at least five days. Both bronchitis and asthma result in less air than usual entering the lungs, and both can create excess mucus (coming from the nose and sinuses) or phlegm (produced by the lower lungs). But while asthma causes airways to narrow due to inflammation, bronchitis causes cells to become inflamed as the immune system fights infection.
Bronchitis, whether viral or bacterial, commonly lasts one to three weeks and clears up on its own. By contrast, asthma is a chronic condition involving damage that cannot be repaired—and symptoms can flare in response to triggers such as pollen and changes in weather. Frequent respiratory infections, however, can also lead to chronically persistent bronchitis.
The two conditions can also occur together in “asthmatic bronchitis”—with bronchitis making symptoms worse in those who have asthma. In addition, “exercise-induced asthma” occurs in about 90% of people with the condition but can also arise in those without asthma. “Reliever medicine” taken before exercise can help both groups.
Deadly sudden asthma attacks are rare—and more likely to occur in asthma sufferers with a history of sudden attacks. In a small study, deadly attacks occurred in the presence of high levels of specific allergens that activated an immune system response, in several cases involving soybean dust —in the Minnesota farmlands and at docks receiving soybean cargoes. Most severe asthma sufferers carry an EpiPen, a device containing epinephrine that spurs quick recovery—but only if bystanders know they should search for the pen and call for emergency help.
I had always been hesitant to dial 911—even when my young son had a high temperature in the early morning hours with wintry weather threatening. On the evening when someone slipped on ice in our driveway, I called 911 only because the person wanted me to. After inspecting the ankle, the EMTs told me they suspected a compound fracture, which comes with a high risk of going into shock and requiring emergency help. Then they carried the patient out on a stretcher.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
GOOD NEWS about Covid keeps getting better—notably as vaccinated individuals contract the virus but generally have less severe symptoms. And as of last week, DC-area “community levels” are low, based —per 100,000 population, in the previous seven days–on new Covid-19 hospital admissions; percent of staffed inpatient beds occupied by patients with confirmed cases; and new Covid-19 cases.
What may be the best news involves recent reports that existing drugs may help treat the “brain fog” affecting many people after a Covid infection. Another result of the enormous research money and effort devoted to Covid is the recent understanding of genetic mutations that may help protect individuals against Covid infection and may lead to better vaccines, as well as an increasing ability to predict and prepare for future evolutions of Omicron variants.
Winter preparedness is the U.S. government’s latest watchword for the Covid pandemic—making free tests once again available at Covid.gov as of this week and promising to alleviate strains on the health care system “if necessary,” one government official told ABC News. “We know what to do in this moment. We have the tools and infrastructure and know how we need to effectively manage this time.”
Sore throat is the now most frequently reported symptom for the latest circulating Omicron variants, followed by runny nose and blocked nose —while the shortness of breath and fever reported toward the beginning of the pandemic have become less common. And while an unusually early flu season may also be peaking early, current Covid symptoms are similar enough to those of flu— notably fatigue and headaches—as well as to RSV that physicians recommend testing before making decisions about treatment.
Less good news comes from rising nationwide levels of cases, hospitalizations and deaths. Last week, all five New York City counties met the CDC threshold for “high community spread” (same definition as above); and infections caused by three viruses —Covid, RSV and flu—reached high enough levels that indoor masking was “strongly” recommended, though not yet mandated.
In addition, the recent mortality risk from Covid has skewed “more dramatically” toward those 65 and over —the age group now with 90% of all Covid-related deaths despite a 94% vaccination rate, writes David Wallace-Wells in the New York Times. Wallace-Wells blames public health messaging that “protection is a choice” as well as “treatments like Paxlovid…criminally underutilized given their efficacy in vulnerable populations.”
(According to the latest thinking, the recurrence of symptoms that can follow a course of Paxlovid is, in fact, “Covid rebound…a brief return of symptoms that starts about two to eight days after you tested negative or stopped feeling sick,” according to Cedars-Sinai. Rebounding symptoms occur in about 10% of people following Covid infection—and while more prevalent in those who have taken Paxlovid, they are not caused by the drug.
But Paxlovid may also be an example of “drugs [developed] for a world of Covid virgins and now that world is gone,” writes pathologist Benjamin Mazer in The Atlantic. Early groundbreaking research, notably on vaccines, involved homo uninoculatus uninfectus, a person who has neither gotten sick with Covid nor ever taken a vaccine—leading Mazer to lament that “we have reached a turning point in our pandemic expertise where some of the astounding progress made since 2020 has started to decay.”
Covid “superdodgers,” on the other hand, have given researchers an important boost in the search for genes that might be protective—similar to those previously found for norovirus (that causes vomiting and diarrhea) and HIV, which led to new vaccines. In the case of HIV, Rockefeller University pediatric geneticist Jean-Laurent Casanova told NPR, one mutation dramatically lowers the risk of symptoms because the virus enters the bodies but “slides off their cells, ‘like water sliding off a glass window.’”
Covid protection for people who have dodged the virus to date may come from several mutations, including one on the HLA gene that spurs the immune system response. According to NPR, “Having one of these mutations would make you a sort of Covid mini-dodger. And perhaps that finding will…lead to a vaccine that does what everyone wishes our current vaccines would do: turn everyone into a Covid superdodger.”
Better protection against Covid may also come from new studies on the evolution of Omicron variants, German computational biologist Moritz Gerstung told New York Times reporter Carl Zimmer. Omicron’s lineages have been acquiring mutations that threaten “what has been one of the most important defenses against Covid: monoclonal antibodies [notably, the drug Evusheld that helps protect people with compromised immune systems],” writes Zimmer. But, Gerstung told him, the new findings have “made me very hopeful..an instance of how one could basically get ahead of the game.”
Finally, Yale University researchers studying “brain fog” in people with long-haul Covid found that drugs used to treat ADHD and traumatic brain injury (TBI) “can mitigate or even eliminate” the symptoms. Linked to inflammation in the brain similar to that seen with TBI, brain fog can include lack of mental clarity, poor focus and concentration, memory problems, difficulty with multi-tasking and more that lasts months or longer following the original Covid infection.
Most worrisome is that “even mild cases of Covid-19 set off enough inflammation to produce impairments to cognition and brain health,” writes retired Harvard public health expert William Haseltine in Forbes. Research on mice, as well as on blood samples from people with long Covid, found compounds involved in inflammation in both the blood and fluid surrounding the brain and spinal cord.
The two-drug regimen “successful in relieving brain fog” in a small group of patients with long Covid included the antioxidant NAC (N-acetylcysteine), available OTC, used in treating TBI and also taken by many hoping to stave off the effects of aging; along with guanfacine, which has been effective in treating ADHD—as well as TBI and PTSD.
Promising results from the regimen may also help patients with other inflammatory conditions. The Yale researchers saw cognitive benefits in one patient with MS—and, exciting for sufferers of other post-viral syndromes, in one post-Lyme patient. With so much research money and effort focused on Covid, hopes run high that further advances in protection and treatment could diminish fears about catching the virus—enough finally to make this coronavirus a benign threat similar to seasonal flu.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
DIETARY recommendations seem to change so often it can be hard to keep track of which ones, such as the currently popular intermittent fasting, are backed by high-quality evidence. In the past week, for example, the Washington Post highlighted two surprising or unfamiliar dietary reports — one, that previously villainized cheese may be protective against cardiovascular disease and type 2 diabetes.
The second is that the USDA’s MyPlate nutrition guidelines, which replaced the food pyramid in 2011, remains unfamiliar to 75% of Americans and affects daily diets of fewer than 10% of adults. On the other hand, people are becoming more aware of the benefits of tailoring diets to individual needs, as well as general advice for those over age 50 to up their daily consumption of protein.
That “obesity is not a personal failing” may, however, remain the most difficult nutrition-related concept for Americans to accept. Writes Julia Belluz in a New York Times editorial describing the recent three-day London conference of obesity researchers: “No presenter argued that humans collectively lost will power around the 1980s, when obesity rates took off…in much of the world. Not a single scientist said our genes changed in that time.”
“All the carbohydrates and fat in our food today dilute the protein our bodies need, driving us to eat more calories to make up for the discrepancy,” proposed one presenter. Echoed another: “eating patterns heavy in carbohydrates are uniquely fat promoting.” Some experts mentioned potential contributions of ultraprocessed foods and the toxic substances they may contain. With more than a thousand genes and variants discovered that increase a person’s obesity risk, conferees agreed: “As long as we treat obesity as a personal responsibility issue, its prevalence is unlikely to decline.”
The popularity of intermittent fasting (IF)—limits on eating to windows of time within each day of 12 hours or less, or one or more days each week—comes from its focus on when to eat rather than what, making IF easier to follow for both weight loss and improved health. By contrast, alternatives such as calorie-restriction diets have a high dropout rate, while the best research-supported diets for health benefits—notably the Mediterranean diet—require keeping track of a variety of food choices.
“The hypothesis behind time-restricted eating is that circadian genes that are thought to increase metabolism are turned on during daylight hours,” Wellness and Weight- Management Co-Director at Brigham and Women’s Hospital in Boston, Caroline Apovian, told New York Times (NYT) writer Gina Kolata. But the most recent research found that time restrictions produced no improvement in “such risk factors as blood glucose levels, sensitivity to insulin, blood lipids or blood pressure.”
In the study of 139 women with obesity, all on low-calorie diets of 1,200 to 1,500 calories a day, half restricted their eating to an eight-hour window between 8am and 4pm while the others did not—with no significant difference between the groups in either weight-loss amount or risk factors. According to UCSF diet researcher Ethan Weiss, “these results indicate that caloric intake restrictions explained most of the beneficial effects.”
Limiting hours of eating may still, however, be the best way for many people to restrict the total number of calories they consume. What may be less well known is the “typically high dropout rate in weight loss studies using IF,” according to Colorado State University food sciences writer Eliza Venetis, “which demonstrates how hard it is to stick to IF in the long run.”
For individuals unable to lose weight with diet, a recent alternative is drugs approved for specific diseases like diabetes. One drug, semaglutide, has different brand names—as well as price tags and insurance coverage—to enable its marketing for either diabetes or weight loss. And the diabetes drug metformin has helped with weight loss and may also slow aging.
MyPlate recommendations emerged from years and millions of dollars spent on research. Despite poor promotion, the general recommendations from MyPlate are better known: Consume about half of daily food in fruits and vegetables; and eat fewer carbohydrates and more fats—notably more unsaturated fats, such as nuts, seeds and fatty fish like salmon.
Increasing daily protein intake, meanwhile, has been garnering more support, especially for those over 50—and especially during stressful periods when “aging bodies process protein less efficiently,” writes Judith Graham for Kaiser Health News. Graham cites a 23-year study showing “older adults who consume more protein are less likely to lose functioning,” and she recommends animal protein that “contains all nine essential amino acids that our bodies need”—but admits that, with a little effort, these can be obtained from plant protein as well.
Eat 30 to 45 grams of both protein and “total carbs” per meal to stave off muscle loss is the AARP recommendation from a series of articles—and consume protein early in the day. From the AARP-published The Whole Body Reset by Stephen Perrine: “Studies show that older folk who fail to get 25 to 30 grams of protein in the morning are likely to stay in muscle-loss mode all day.” Other recommendations include strength-training and eating lots of fruits and vegetables.
Misinformation extends to all consumption, such as the goal of drinking eight glasses of water a day. Updated advice is to drink water when you’re thirsty, and it’s better to do so before or after meals versus while eating when water can dilute digestive juices. Drinking water can, however, can help prevent stomach growling. The misperception is that hunger is the cause, whereas such rumbling or gurgling noise is a sign of digestion underway.
And as for cheese, studies on health benefits have upended earlier blame for coronary vascular disease (CVD) on saturated fats. According to a 2019 University of Copenhagen study of 136,384 individuals from five continents, the results “clearly demonstrated that dairy consumption…is associated with lower risk of mortality and major CVD events.”
“Body neutrality” —accepting and respecting different kinds of bodies—might be the most important nutrition goal for the future, based on the obesity conferees’ conclusion that as long as “the individual choice bias dominates…fat shaming promotes weight gain and harms. At least some of obesity’s negative health consequences are thought to be driven by stigma and discrimination which results in poorer health care.”
Growing up with a grandmother who praised “eating to live” versus “living to eat,” I developed the knee-jerk reaction of criticizing heavier bodies—along with the flip side, commenting positively when someone appeared to have lost weight. While working on “body neutrality,” I am trying to figure out how to squeeze the many MyPlate recommendations into daily consumption—as well as how to eat more protein, especially at breakfast time.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
Much of the inspiration for researching sound’s effects on the body comes from its potential benefits for sleep and for pain and anxiety relief. While the emotional effects of sound bathing might appear easier to assess than those of the forest, because of the objective measurements of decibel (loudness) and Herz (frequency, or vibration), the supporting evidence is not much more definitive.
Symphonic music’s ability to block pain is among the most measurable effects of sound, seen in mouse studies led by neurobiologist Yuanyuan Liu at the National Institute of Dental and Craniofacial Research. After researchers artificially interrupted the connection between the auditory cortex and the thalamus, which is the central hub of sensory processing in the brain, the mice appeared numb: when prodded, they didn’t flinch or pull their paws back.
The numbing occurred only when music was played quietly—at around 50 decibels, barely above the sounds of background noise—while at louder levels, the mice’s paws became almost three times as sensitive. Numbing effects were similar using both pleasant and dissonant symphonic music, as well as white noise—all of which, at these low sound levels, create a sort of buzzing sound. Said Harvard neurobiologist Clifford Woolf, “Many would have anticipated you need to listen to Mozart to get pain relief. But maybe all we need is to give patients a tiny level of buzzing noise.”
Dentophobia or odentophobia —“extreme fear of going to the dentist”—inspired an Indian study of 50 dental patients undergoing tooth extraction. For the 25 patients who listened to music, anxiety levels decreased as did blood pressure and heart rate. But the effects occurred only when the music was familiar —religious music for these patients, whereas classical music caused their levels to rise.
Familiar music, however, “might recall certain pleasant memories associated with the music…and therefore is responsible for the reduced anxiety,” the researchers suggested. (Experts warn that “true phobias, stronger versions of the common fear, require different and sometimes more intensive measures,” such as weighted blankets that apply deep-touch pressure.)
“Welcome to the cult of brown noise” began a recent New York Times article on physiological effects of “immersive” sound frequency combinations found in white, brown and pink noise—that “may help the brain to focus, sleep or relax especially for people with ADHD,” writes Dani Blum. Like white noise but with a lower, deeper quality, brown noise is a “category of neutral, dense sound that contains every frequency our ears can detect” with effects that can be smothering.
“Noise that is just stimulating enough to activate the brain but is not overwhelming” can help block background noise as well as internal chatter, such as worrisome thoughts, according to Blum. Pink noise plays at lower frequencies than white noise but louder; violet noise includes higher frequencies that can make a hissing sound; and gray noise “sounds similar to white noise, but is smoother.” Pink noise in a small study led to deeper sleep—though some researchers trace the effects of these sounds simply to drowning out annoying noise such as traffic. And because the sound combinations can bleed into each other, noted Regis University pharmacy professor Daniel Berlau, “it’s not as scientific as people would think.”
For the most intensive auditory effects, “sound baths” can combine a mix of different instruments “because each gives off different frequencies or vibrations,” according to yoga teacher Christy Maskeroni Price. Small studies suggest health benefits such as lowered heart rate and heart rate variability following sound baths may reflect reduced stress and anxiety—while others suggest “sound baths” are more likely to provide a spiritual experience in contrast to the medical effects of music therapy.
“Solfeggio frequencies” refers to “specific tones of sound that help with and promote various aspects of body and mind health,” according to the BetterSleep blog. “Musically speaking, the frequencies [begin] at 8Hz and working up the musical scale octave by octave until the C note is vibrating at the 256 Hz frequency and the A note is vibrating at 432 Hz.” (The frequency of the highest piano note is above 4000 Hz, while flute sounds are closer to 2100 Hz and most songbirds’ chirping falls between 2000 and 3000 Hz.)
Different solfeggio frequencies played in varying combinations create vibrations that purport to heal specific ills. Frequencies at Apple’s solfeggio site, for example, begin with help for trauma, fear and negative energy at 285 Hz, 396Hz and 417 Hz respectively—with links to listening experiences for each one.
Different people react to sound baths in different ways, however, with feelings that range from especially relaxed to a boost of energy. But compared to virtual sound baths, being in the room with musical instruments offers a more direct experience of the vibrations, according to Price. In-person sound baths are available at centers for alternative health or yoga, as well as at pop-ups listed as they arise.
To experience the sound bath of the Integratron near Joshua Tree National Park, people travel from around the world and reserve months in advance. According to the Integratron site, “sonic sessions” in its wooden dome include a sequence of 20 quartz crystal singing bowls with “each bowl keyed to the energy centers or chakras of the body.”
Because the Integratron has no waiting list, those hoping to snag a place from no-shows arrive early to wander through the surrounding desert garden. Visiting Joshua Tree with a friend, we eventually obtained two passes. But we found it hard to separate effects due to the softly chiming bowls from those of lying on soft mattresses under the beautiful dome—or of having already spent several days on a desert vacation. We did emerge very relaxed—as well as energized for an afternoon desert walk, plus a night of live music in the nearby mountains.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
“Forest bathing” and “sound bathing” are activities with specific intentions and parameters. While skeptics question how they’re different from simply turning on music or walking among trees, both activities come with goals and guidelines, along with research supporting their benefits—hence, our two-part series.
Forest bathing—which originated in Japan as shinrin-yoku—led practitioners in one study to develop a “smaller self.” In selfies taken over an eight-week period, the heads of the forest bathers gradually became smaller in relation to their backgrounds—interpreted by the researchers as turning attention away from the self. As UCSF neurologist Virginia Sturm explained, while there is no science confirming what smaller heads accurately reflect, the group reported feeling happier, less upset, more socially connected than the control group —and showed a “small but significant improvement in well-being.”
All 52 volunteers in the study received directions to walk outdoors for 15 minutes weekly, taking selfies and writing online assessments to document their experiences. The group of forest bathers, who were also asked to walk in a new place when possible and pay attention to details “with fresh, childlike eyes,” became adept at “discovering and amplifying awe,” according to Sturm. The forest bathers paid less attention to themselves, while at least one person in the control group reported worrying about her to-do list.
“Awe—a positive emotion…in the presence of vast things not immediately understood—reduces self-focus [and] promotes social connection..by encouraging a “small self,” Sturm wrote in her original report titled “Big Smile, Small Self.” “Awe is partly about focusing on the world outside of your head”—and the study results suggest that cultivating awe diminishes “negative emotions that hasten decline [with aging].” The forest bathers also “displayed increasing smile intensity” over the course of the study.
Shinrin-yoku, or “taking in the forest atmosphere,” is a form of “ecotherapy” embraced by the Japanese beginning in the 1980s, writes Sunny Fitzgerald in National Geographic. Its two purposes: “to offer an eco-antidote to tech-boom burnout and to inspire residents to reconnect with and protect the country’s forests.”
Native evergreens in New York’s Adirondack Park are “both aromatic and release a high concentration of phytoncides—airborne essential oils that provide a natural immunity boost,” according to Fitzgerald, naming this park at the top of her list of five forest-bathing destinations. The phytoncide shower can last for weeks, while the needles of trees that include spruce and eastern hemlock can produce a tea “rich in antioxidants and Vitamin C.”
“Become more resilient” is the headline for a short AARP forest bathing recommendation: “20 minutes among the trees…exactly how much time you need in nature to reduce your level of stress hormones significantly.” A 2017 meta-analysis that included 40 interventional studies found “increased greenspace exposure associated with decreased salivary cortisol”—along with reduced incidence of stroke, asthma and coronary heart disease.
And, although not specifically forest bathing, 120 minutes spent on “recreational nature contact,” compared to no nature contact, led to a significantly higher “likelihood of reporting good health or high well-being,” according to a report in Nature. The seven-day study that included almost 20,000 participants in the “Monitor of Engagement with the Natural Environment Survey” between 2014 and 2016 found that “positive associations peaked between 200-300 minutes a week,” regardless of whether these took place over 28 to 42 minutes per day or one long visit with several shorter ones per week.
“The key [for forest bathing] is to practice mindfulness…focus on what your senses are taking in,” according to the KaiserPermanente website. To begin, “take a few deep breaths and center yourself… sit and watch how the trees sway in the wind or simply walk around… at a leisurely pace and without a specific destination in mind.”
For awe walks, look at your surroundings with fresh eyes or take a new walking path, advises the Kaiser site: “Remember to look for moments that make you feel amazement—or awe.” And pay attention to what your senses are taking in—whether it’s the scent of clean ocean air or a chorus of chirping birds.”
I take walks in the nearby forest but usually listening to music or accompanied by friends. On the few walks I have taken alone in silence, however, I have become aware of the changing light, the colors of leaves, the sounds of water rushing in the creek below. I am considering making a New Year’s resolution to plan more forest baths—or I might start more tentatively by wishing to try that, every now and then.
(Stay tuned next week for Sound Bathing.)
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
THE BACTERIAH. pylori “lives in half of the world’s people,” according to New York Times food reporter Priya Krishna, who has “never known what it means to have a normal digestion.”After a childhood diagnosis of acid reflux, Krishna spent years taking antacid tablets that didn’t help —followed by testing for food allergies that turned up nothing. Krishna writes that, now that she’s dining out a few times a week for work, afterwards, “more often, I’ll be pinned to the couch for hours with a stomachache.”
Heliobacter pylori made a big splash in 1984 when Australian gastroenterologist Barry Marshall consumed a petri dish full of the bacteria in an effort to prove they were the cause of stomach ulcers. After three days, Marshall experienced abdominal symptoms; after eight, he developed severe gastritis confirmed by GI testing. In 2005, Marshall and colleague, J. Robin Warren, won the Nobel Prize in Physiology or Medicine for their discovery that H. pylori caused peptic ulcers.
Until then, doctors had blamed lifestyle choices—stress and diet—for dyspepsia (indigestion) and peptic ulcers, sores in the upper digestive tract. The best recourse for sufferers was to avoid spicy and acidic foods, and alcohol– restrictions that kept stomach ulcers in the news, especially around food-focused holidays like Thanksgiving.
Once H. pylori became the clear culprit—with most gastritis remedied using easily available treatments that ranged from antacids and proton pump inhibitor drugs (PPIs) to antibiotics—reports of stomach acid and peptic ulcers died down. Writes Times reporter Krishna, “H. pylori isn’t getting the same public attention as irritable bowel syndrome, the gut issue currently making the rounds of Tik Tok among users who identify as ‘hot girls with I.B.S.’”
In the current pandemic, however, people infected with H. pyloriappear more susceptible to SARS-CoV-2 infection as well as more likely to have severe Covid symptoms. Based on Chilean research, H. pylori in the gastric mucosa can increase expression of the specific receptors that allow the virus entry into cells— and can cause inflammation similar to that seen with diseases such as diabetes that elevate the risk for severe Covid.
Most of the 30-40% of people in the U.S. whose guts harbor H. pylori contracted the infection during childhood, and most have no symptoms. The most common signs of H. pylori are stomach pain and sensations of burning that can last from a few minutes to several hours and can travel away from the center of the stomach. Other symptoms are bloating and feelings of fullness, belching, heartburn, unexplained weight loss and chest pain. One distinctive symptom is hunger or an empty feeling in the stomach one to several hours after eating.
H. pylori is responsible for most peptic ulcers—both gastric, in the stomach, and duodenal— as well as for most cases of chronic gastritis, an inflammation of the stomach lining. But gastritis can have other causes, most commonly the use of nonsteroidal anti-inflammatory drugs (NSAIDs), but also the autoimmune inflammatory bowel disease (IBD) and viral infections, such as cytomegalovirus.
While symptoms of gastritis may be mild or intermittent, the main worry for sufferers is the risk that chronic inflammation can be an “important initiating and promoting step of gastric cancer,” according to the Chilean researchers. Stomach cancer is the second leading cause of cancer-related deaths worldwide, and its prevalence may be increasing. Among individuals infected with H. pylori, “approximately 10% develop peptic ulcer disease [and] 1 to 3% develop gastric adenocarcinoma, according to Vanderbilt University gastroenterologist Lydia Wroblewski and colleagues.
Because of the cancer risk, upper endoscopy— placing a tube through the mouth into the digestive tract to allow direct observation of the mucosa and collection of a biopsy sample—is the “gold standard investigation for confirmation of H. pylori” for individuals over 60 years old, for those using NSAIDs and for anyone with “alarm symptoms.” These can include a family history of upper GI malignancy, feelings of fullness, iron-deficiency anemia, unexplained weight loss, recurrent vomiting, difficulty swallowing and GI bleeding.
For younger patients who have stomach pain that suggests peptic ulcer disease (PUD) lasting longer than one month, less invasive testing and treatment can counter the risk of recurring inflammation and symptoms. In addition to serum and stool testing, there’s the urea breath test, which involves swallowing a liquid that contains urea; in the exhalation, the presence of H. pylori converts urea into carbon dioxide. Because the breath test can be expensive and people worry about radioactivity in the solution, however, few emergency departments or doctors’ offices have the ability to perform the test.
Once H. pylori colonizes the gastric environment, “it persists for the lifetime of the host,” writes Wroblewski, “suggesting that the host immune response is ineffective in clearing this bacterium” without treatment. The first “standard outpatient therapy” is the so-called empiric PPI trial— using proton pump inhibitor drugs to reduce inflammation and counter symptoms, which can obviate the need for testing. Following detection of H.pylori, though, only antibiotics can produce a complete cure.
“Treatment for H. pylori infection is challenging,” Mass General primary care physician Wynne Armand writes in a HarvardHealth blog. “The cure rate depends on picking the right combination of…three or four medications [taken] multiple times a day for 14 days.” The choice of antibiotics varies according to antibiotic resistance in the patient’s region as well as which antibiotics they have taken in the past—with the likelihood that their H. pylori has become resistant to these.
I have occasional indigestion and GERD, as do many of my acquaintances—though our symptoms sound less debilitating than those of Times food writer Krishna. Most of us do not eat complicated restaurant food on a regular basis. Still, I am curious whether the easier, more accessible testing methods currently under development will one day become part of annual physical exams for many more people like us.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
“WHEN EVIDENCE Says No, But Doctors Say Yes” headlined a 2017 collaboration between the Atlantic and investigative journalists at ProPublica that investigated unnecessary and potentially harmful medical interventions, including sinus surgery and arthroscopic knee surgery. While other “evidence” recommends many of these procedures, poor communication and deteriorating trust in science can make it hard to keep track.
Blame for overuse of the disputed interventions goes to greedy doctors, pushy patients, fear of malpractice and flawed science. But while the Atlantic article makes a good case against some oft-performed procedures, like stents implanted to treat stable angina, many of the other treatments it mentions remain controversial, such as daily aspirin to lower risks of heart attack, stroke and colon cancer; and hormone replacement therapy (HRT) to counter heart disease in post-menopausal women. Also up for grabs are less familiar regimens, such as the need for prophylactic antibiotics before dental surgery on those with artificial joints.
For public health interventions, such as cardiopulmonary resuscitation (CPR), the Atlantic laments the lagging adoption of compression-only CPR–without the addition of rescue breathing. According to emergency medicine experts, however, while compression-only CPR works well in cases of sudden, “primary” heart attack, rescue breathing remains “essential” in cases of secondary arrest—that can accompany near-drowning, opioid overdose or suffocation—to get oxygen moving into the body.
The Atlantic article refers to the RightCare Alliance that “seeks to counter a trend: increasing medical costs without increasing patient benefits…Even if a drug you take was studied in thousands of people and shown truly to save lives, chances are it won’t do that for you.” Similar organizations include the Lown Institute, the Cochrane Reviews and Do No Harm.
“The most widely prescribed medications do little of anything meaningful, good or bad, for most people who take them,” concludes the Atlantic. RightCare Alliance is currently waging a campaign against the newly FDA-approved drug Aduhelm for Alzheimer’s treatment, which “has not been clinically proven to work [to prevent decline of cognitive function] and will cost $56,000 a year.”
The “missionary waste-hunting zeal of the ‘less is more’ movement,” however, is how Harvard Medical School professor and cardiologist Lisa Rosenbaum, writing in the New England Journal of Medicine, describes such organizations. Rosenbaum noted the “suspect” methodology of a major study that found 30% waste in U.S. health care, and criticized the less-is-more movement for putting “dangerous pressure on physicians to abstain from recommending some helpful treatments.” To explain growing support for less-is-more, she blamed erosion of trust in medical science as well as in physicians and their recommendations.
Many treatments most deplored by the watchdog groups, meanwhile, remain as recommendations by reputable medical organizations. According to Mayo clinic sites, for example, daily aspirin “may lower the risk of heart attack and stroke…depends on your age, overall health and history of heart disease;” while HRT treats common menopausal symptoms and has “been proved to prevent bone loss and reduce fracture in postmenopausal women [depending on] type of therapy, dose, how long the medication is taken and… individual health risks.”
The Atlantic article highlights criticism of arthroscopic knee surgery to clear out damaged tissue and shave cartilage on the meniscus as “one of the most popular surgical procedures in the hemisphere… at a cost of around $4 billion a year [but] does not work for the most common varieties of knee pain.” Arthroscopic surgery may also increase the risk of knee osteoarthritis, the story contends. It mentions studies showing that physical therapy alone performed as well as that combined with surgery; and a Finnish study that found “sham surgery” —cutting into all participants’ knees, including those in the control group who had no work done (to avoid the placebo effect) —performed as well as the real surgery.
And RightCare Alliance’s report on ESS (endoscopic sinus surgery) to alleviate sinus infections pointed to “an open secret within otolaryngology that patients are being abused with unnecessary surgery,” according to Northwestern University otolaryngologist Arthur Curtis. “None of the usual sources… recommend ESS for most of the conditions for which it is utilized,” including nasal allergies, non-allergic rhinitis and nasal polyps.
Opposing research, however, points to positive results for both surgeries. For ESS, the surgery’s “primary goal [is] to improve the quality of life of patients who have failed medical therapy…prevent complications and potentially alter the natural course of the disease,” according to Greek researchers. Their study of almost 1,000 patients who had ESS surgery after 12 weeks of resistance to medical (antibiotic) treatment found benefits in postoperative quality of life and especially in “emotional/general symptoms.”
When a group comprised of patient advocates as well as clinicians focused on underuse—along with overuse—of medical procedures, almost half of the 10 recommendations dealt with improving communication to patients. The panel noted its work “to steer patient and provider views away from rationing and…to improve the overall quality and value of care provided.” (The first recommendation, to deal with a major complaint of hospitalized patients as well as a potential impediment to healing, was to “implement programs designed to promote sleep in the inpatient setting.”)
Over the years when I had meniscus and then sinus surgery, our trusted family pediatrician said he’d heard these “didn’t work.” But for me, both surgeries put an end to miserable difficulties: sinus surgery, to more than five years of infections causing pain and making sleep almost impossible; and meniscus surgery, to shooting pain down my calf at any unexpected movement —every time I tried to play catch with my sons.
What persuaded me to have both surgeries was advice from people I trusted. For my knee, a physical therapist who had helped everyone in my family explained that a key variable in deciding to have surgery is whether the pain interferes with an activity important to me. For sinus surgery, a reliable good friend who’d suffered similar infections told me how surgery relieved her suffering. More important to me than large population studies that discouraged these surgeries was having advice from two people who were both familiar with my particular knee and sinus problems—and who knew me.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
IN A DC-area creative writing workshop, a young woman reacted to another participant’s essay using what sounded like words but made no sense at all. At the break, after the teacher left the room with the woman, someone called the problem “word salad.”
Word salad most often refers to the nonsensical language that can result from aphasia—hence its clinical label “jargon aphasia” —which involves difficulties with expressive (producing) or receptive (understanding) language. Different forms of aphasia depend on which part of the brain is affected—most often due to stroke, as in the case of Pennsylvania U.S. Senate candidate John Fetterman. Aphasia can also result from physical damage, for example, the gunshot that tore into the brain of former Arizona congresswoman Gabrielle Giffords.
In news reports on the speech difficulties of Giffords and Fetterman, medical experts have struggled to convince audiences that aphasia does not indicate impairment of the neurological functions involved in cognition. Instead, aphasia usually results from damage limited to the two distinct language-producing regions of the brain, Wernicke’s and Broca’s areas. What can be confusing in discussions of aphasia, however, are different uses of the word cognitive.Cognitive functions —such as remembering and reasoning—play important roles in producing and understanding language and remain unaffected in most cases of aphasia.
Aphasia, however, has the label “cognitive disorder”; and severe aphasia can involve damage in the language regions, thus becoming one of the impairments of dementia. For actor Bruce Willis, reports of aphasia came years after co-workers noticed “loss of mental acuity,” according to the LA Times. Willis’s behavior had provoked questions about whether the actor was “fully aware of his surroundings on set.”
Most common, Wernicke’s aphasia can produce long, complete sentences that have no meaning and can include made-up words as in “word salad” —with the example, “You know that smoodle pinkered,” according to the National Institute on Deafness and Other Communication Disorders (NIDCD) . Wernicke’s is categorized as “fluent” aphasia, while the speech of nonfluent Broca’s aphasia can require great effort, emerge in short phrases and omit small words such as “and” and “the.” “Walk dog,” for example, means “I will take the dog for a walk.” Sufferers of both kinds are often unaware that their speech is unusual.
John Fetterman’s use of closed captioning to improve his speech is an important clue that his cognitive abilities are unaffected. As is common with Broca’s aphasia, Fetterman’s speech stumbles are often paraphasic errors, using an incorrect word that sounds like the intended word they are trying to say —such as “emphetic” instead of “empathetic.”
Damage from a stroke—which can be pinpointed using MRI or CT scans—is most often limited to the brain’s left hemisphere, the location of the two language centers. The most common kind of stroke, transient ischemia attack (TIA), can interrupt blood flow to the brain for as little as a few seconds, which affects language abilities for just a few hours or days.
“What” and “chicken” were the only two words that Gabrielle Giffords could say in the weeks after she was shot in Tucson, according to an editorial by Giffords in the Washington Post. Even when she practiced telling her husband “Happy Birthday,” she couldn’t “help adding ‘chicken,’” she wrote: “Happy Birthday—chicken!”
“Though my cognition— my understanding and intelligence—is unaffected by my aphasia, sometimes that is not clear to new acquaintances because of my speech,” Giffords writes. She explains learning about “functors”—the small words, including prepositions, conjunctions and articles— which her aphasia causes her to drop. In an effort to compensate, she communicates using as few words as possible and explains: “Words are precious to me.”
“Global” aphasia caused by severe injury or stroke, on the other hand, damages extensive portions of the brain, along with the language areas. Severe damage can result in anomic aphasia, or anomia, with the speaker understanding words and sentences but struggling to come up with the names of objects. What’s called primary progressive aphasia, on the other hand, involves deterioration in parts of the brain responsible for language —that can lead to further brain degeneration, including memory difficulties and the inability to manage daily activities, explained Giffords’s Tucson-based speech and language pathologist, Fabi Hirsch.
The struggles of aphasia sufferers like Giffords to make themselves understood can cause mounting frustration. When a member of my extended family, G.K., developed anomia, we explained that she was “losing her nouns,” and we became pretty good at figuring out what word she was searching for. But conversations became more difficult for her, and probably tiring; and she began speaking less often. G.K’s eventual diagnosis of dementia was an example of aphasia that eventually leads to cognitive impairment.
A specific frustration for those with jargon aphasia is the similarity of their garbled speech to that of schizophrenia patients—including poverty of content, perseverative speech and delays in responding, write Duke psychiatrist Zachary Paul Lane and colleagues. But among differences between the two, the psychiatrists explain, schizophrenia patients often speak with flat intonation and unusual voice quality. Compared with aphasia sufferers, schizophrenics generally “display a greater mastery of language, employing more complex word usage and better use of lexical rules for sentence structure;” also, their speech is “more circumstantial, more tangential and tends to have persistent themes, sometimes becoming bizarre or delusional.”
When I participated in the writing class with the word-salad woman, and later when I spent a lot of time with G.K., I had no understanding of their challenges. In both cases, despite wishing to be thoughtful about disabilities, I was impatient. Now that I know more— and have lost a few of my own nouns—I hope to show more kindness to anyone who struggles to speak.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
“WINTER is coming” is the ominous-sounding phrase weaving its way through autumn Covid news—like echoes of the oft-repeated threat in Game of Thrones. For now, U.S. Covid levels are inching up slightly, but hospitalizations due to Covid are increasing in the New York region, and the new subvariants of BA.5—BQ.1 and BQ.1.1 — appear more transmissible than earlier variants.
“Dr. Fauci is sounding the alarm about a pair of “pretty troublesome” Covid variants,” CNBC reported last week. Especially concerning is the “doubling time” of BQ.1 and BQ1.1 —which in the New York region account now for nearly 17% of infections, up from 11 percent two weeks ago—and BQ1.1 has already “sent cases soaring in Europe.”
That current Covid deaths number around 350 a day sounds like such a vast improvement over more than 3,000 a day at the height of the pandemic, but annually deaths come to around 130,000—compared, for example, to the under-30,000 annual average for flu deaths. According to a recent Kaiser Family Foundation analysis, Covid deaths among those 65 and over spiked during last summer—more than doubling between April and July 2022—and continue to remain high.
“The U.S. is woefully under-vaccinated and under-boosted,” according to Scripps Researcher molecular medicine specialist Eric Topol. Although the most recent bivalent Covid booster may not provide better protection than earlier formulations, all boosters add important layers of protection against serious illness, especially in the event of a winter wave.
What makes boosters even more important: The new subvariants appear better at dodging protective antibodies generated by breakthrough BA.5 infections, according to recent Chinese research. But vaccines, notes Carolyn Y. Johnson writing in the Washington Post, “teach the entire immune system [not just antibodies] to fight a virus.”
Overselling the new boosters, on the other hand, may create new problems. Microbiologist and immunologist John P. Moore at Weill Cornell Medicine in New York told the Post: “if you talk up these bivalent boosters as being some kind of super strong shield,” people will believe they can relax precautions.
New warnings of a “tripledemic” focus on three viruses: Covid, with cases rising in Europe and lately New York city; flu, which appears to be striking earlier this fall than expected; and RSV (respiratory syncytial virus). While RSV has infected almost everyone by age two and is most worrisome in babies under six months, the National Foundation for Infectious Diseases calls RSV in adults aged 65 and older “a hidden annual epidemic.”
Similar symptoms for all three are like those of a cold, including sore throat, runny nose and cough—but infection spreading to the lower respiratory tract, sometimes signaled by a “barking or wheezing cough,” can cause more serious illness. Mayo Clinic infectious disease expert Aditya Shah advises testing for anyone who has a respiratory infection that is getting worse—either by healthcare personnel or using the new Labcorp home P.C.R. test for all three viruses (free, mailed via Fedex, with results within two days).
Another worry with new variants concerns Evusheld, a key antibody treatment given to immunocompromised individuals, which appears to be ineffective, or “obsolete,” against the variant BQ1.1.
Good news, on the other hand, comes from wastewater sampling around the country—which can help predict possible spikes in Covid ahead of CDC data. For the past six weeks, testing by Biobot Analytics has shown the amount of coronavirus to be “basically flat.”
Wastewater sampling is one strategy in need of standardization, according to critics of government policies for this pandemic— and in preparation for the next — as are national standards for indoor air quality. And, University of Pennsylvania bioethicist Ezekiel Emanuel told the Post, “We can’t let this moment pass with so few structural substantive, institutional improvements.”
The government’s focus on individual decision-making as its current Covid policy is another target of criticism. Said Cecilia Tomori, director of global public health at Johns Hopkins School of Nursing: “When you make a rhetorical choice like [CDC director Rachelle Walensky recently calling Covid] ‘the pandemic of the unvaccinated,’ you’re really shifting the blame.”
Some experts have, nevertheless, updated suggestions for coping with the newer variants to account for their shorter incubation periods. UCSF infectious disease specialist Peter chin-Hong told the Post: “if you go to a packed bar on a Friday and don’t have symptoms by Monday, it’s unlikely you have the virus.”
Other advice concerns the week before traveling: “Consider a mini quarantine,” limiting time spent in crowds and masking in indoor public spaces, as well as masking “while traveling…even if you’re the only person on a plane or train wearing one.”
For now, individual choice is all we’ve got. I have not been infected with Covid, have had five shots and remain reluctant to eat in crowded public places—with exceptions for family and friends. When visitors arrive from New York or elsewhere to stay with me, I have Covid tests at the front door for each of us to take. Recently, I have joined a new group, the Coviders, and we convene on social media to talk about how we are “still COVIDing.” Still, I fully expect to get Covid any day now.
FLORIDA LAWYER L.M. describes the occasional sensation of not being entirely “there” or present. As she wrote in an email, “I go through the motions . . . trying to be likeable but fearing that I come across as wooden, as if I must playact because I’m so detached.”
People rarely talk about momentary feelings of what’s labeled “common dissociation,” though many have similar experiences from time to time. The most familiar has its own label, “highway hypnosis”: daydreaming or zoning out while driving and not remembering the last few miles of highway. While momentary dissociation can cause difficulty concentrating and memory lapses, the mental health condition called dissociative identity disorder (DID) involves “an involuntary escape from reality that interferes with a work and/or family life.”
Recently claimed by Georgia Republican senate candidate Herschel Walker to explain past transgressions, DID replaces the earlier diagnosis of Multiple Personality Disorder. DID refers to people who have two or more separate identities or personalities that control their behavior at different times.
A key symptom of DID is “missing time,” according to the Atlanta Journal-Constitution—for example, ending up in a location and not knowing how you got there. Herschel Walker has reported having “12 alternate personalities—or alters—including the warrior (who played football), the sentry (who avoided emotional attachments) and the thrill seeker (who played Russian roulette with a loaded gun).”
But dissociation can be a useful coping mechanism for sudden trauma, as when rape victims experience floating above their bodies during the crime or those involved in serious car accidents remember very little afterward. While this kind of dissociation is usually temporary—people regain their normal perspective soon afterward—bouts of DID can also come and go, blurring its differences from common dissociative experiences.
Related to DID along a similar spectrum is depersonalization-derealization disorder. Depersonalization involves feelings of being disconnected or outside your body, as if you’re observing yourself from a distance or sensing that you aren’t real; with derealization, the surrounding world feels unreal or as if you are living in a movie.
In its milder form, dissociative amnesia refers to trouble remembering personal information or facts about your life. Dissociation can also include fugue states, “experiences where you travel or wander with no memory of what happened; blank spaces in your memory; or sudden lapses in recent memories or skills,” according to psychcentral.
Disorders of dissociation like DID affect from 1% to 3% of the population, occur more frequently among women and most often develop in response to physical or emotional abuse occurring in early childhood. While physical or sexual abuse is the most obvious and dangerous, emotional abuse or neglect by parents—reported by some 14% of Americans—can range from insulting or swearing to terrorizing, threatening to physically harm or otherwise making a child feel afraid.
DID most often originates from parental abuse that occurs before age 9, during the “not me” magical thinking stage of development when children personify dolls and stuffed animals, explains McLean Hospital psychiatrist Milissa Kaufman. “A child doesn’t have many other ways to cope. They can’t go to their parents, since that is the origin. . . . They feel like there are other people inside of them, and they can’t tell anybody.”
“Captivity, which brings the victim into prolonged contact with the perpetrator [including an abusive parent], creates a special type of relationship, one of coercive control,” according to trauma specialist Judith Herman. Herman describes “the psychological impact of subordination to coercive control” whether the context is public and political, or private—including domestic relations.
“People with dissociative disorders report the highest occurrence of childhood abuse and/or neglect among all psychiatric diseases,” writes University of Toledo psychologist Matthew Tull on verywellmind. And whereas PTSD can develop after a single traumatic experience, “repeated episodes of physical, emotional or sexual abuse . . . before the age of 9 years [are] most strongly associated with the development of dissociative disorders.”
On MRI brain scans of young adults who experienced childhood abuse or neglect, “the most obvious changes were in the brain regions that help balance emotions and impulses as well as self-aware thinking,” according to psychiatrist Martin Teicher and colleagues at Harvard and Northeastern University.
Potential effects of these brain changes include “being constantly on alert and unable to relax . . . weakened ability to process positive feedback . . . problems coping with stressors.” Because the damage originated in early childhood, most experts consider the best treatment to be talk therapy, such as cognitive behavior therapy or psychotherapy.
Signs of someone faking or mimicking DID include blaming bad behavior on the disorder’s symptoms, exaggerating symptoms and lying, and showing little distress regarding the apparent diagnosis. For most people with a DID diagnosis, on the other hand, each personality has no apparent awareness of the other(s); and even those experiencing momentary dissociation struggle to hide or cover up mild lapses in concentration or memory.
While Herschel Walker has said in past interviews and in motivational speeches that he is healed from DID, he continues to blame alternative personalities for alleged incidents of lying and violence toward women. Walker, who wrote about his battle with DID in his 2008 memoir Breaking Free: My Life With Dissociative Identity Disorder, declined an interview request from The Atlanta Journal-Constitution.
Dissociation joins a host of conditions with symptoms that vary from disabling to common and mild, without interfering with daily life. Other “spectrum disorders” are ADHD and OCD, although autism is the one most often given this label. But being on any spectrum can make an individual worry, even someone like L.M., whose experiences of dissociation are the mildest, briefest, and most common—in the midst of an otherwise productive, happy, friend-filled life.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
MyLittleBird often includes links to products we write about. Our editorial choices are made independently; nonetheless, a purchase made through such a link can sometimes result in MyLittleBird receiving a commission on the sale, whether through a retailer, an online store or Amazon.com.
DIAGNOSED WITH a post-surgical infection, retired DC lawyer —and swing dancer— L.H. raced to the nearby CVS to fill an antibiotic prescription for Linezolid (generic Zyvox), specifically targeted at such infections. But the price at CVS, using her Medicare Plan D prescription insurance, was about $2,000 for 20 pills—down from the $3,000 retail price.
On GoodRx—one of several sites offering drug discounts—however, the price plunged to $41.89 at Giant (and at Safeway, $43.47) as of last week. Even on a discount site, though, the CVS cost remained high—$757.95. A caveat of using drug discounters is that you cannot use medication insurance in any combination payment, and whatever you pay you can’t use toward annual insurance deductibles.
When DC journalist S.G. received a prescription for mirabegron (Myrbetriq) to treat urge incontinence (UI), one form of overactive bladder, the Costco price was around $500/month ($400 on GoodRx). But a similar drug, tolterodine, cost about $40 at Costco. Moreover, it worked well, even when taken every other day and had the added bonus of helping reduce intestinal gas. “The stuff has been a miracle,” said S.G.
Drug pricing is not just out of control but complex—posing often insurmountable challenges for patients at the same time they seek urgent relief and have little ability to research the options. Prescription drug expert Michael Rea, who works with employers to find lower medication costs for workers, told the New York Times: “There’s no chance that a consumer can figure it out.”
“People are shocked to discover they can sometimes get better deals than their own insurers,” according to the New York Times. “Behind the seemingly simple act of buying a bottle of pills, a host of players —drug companies..insurers…—are taking a cut of the profits,” in up to 10 percent of drug transactions or about 40 million prescriptions per year.
“Good Rx is free!” writes thefrugalpharmacist. “Everyone can use GoodRx [even] for your pets.” At no cost to the user, average savings fall close to 50% but can reach 80%—and, with the paid GoodRx gold membership service, up to 95% on some drugs.
The pricing morass has serious ramifications, notably that hotly anticipated new drugs may take even longer to come on the market following FDA approval—at least “several months of negotiations” between insurance companies and the manufacturer, according to verywellmind. An example is the new antidepressant Auvelity— combining Wellbutrin with the ketamine-like drug dextromethorphan—that may be at the forefront of “a potential new wave of faster-acting antidepressants.”
The complexities also make it difficult to assess benefits just conferred by President Biden’s Inflation Reduction Act for those with Medicare Part D drug plan. According to the White House, benefits include lower prescription prices, because Medicare can now negotiate costs; a $2,000 cap on annual drug costs for everyone on the plan; and for diabetics, insulin costs capped at $35 for a one-month supply.
(OTC drugs have not escaped pricing craziness. After years of paying about $1 per pill for Claritin with pseudoephedrine, taken daily from early spring to late fall, I switched to generic Zyrtec GoodSense—$14.10 for 365 pills on Amazon—based on an internist’s recommendation, as well as reports from many others already in the know about this “deal.”)
My first encounter with drug-pricing quandaries involved a new drug, Vimovo, prescribed by a pain physiatrist. Not covered by Medicare, the drug combines a formulation that protects the stomach along with an NSAID, which can cause abdominal pain. My CVS pharmacist, however, explained that the cost to me would be above a shocking $2,000 for a month’s supply; instead, he suggested, he could give me a common, stomach-protecting proton-pump-inhibitor drug for around $10, which I could take along with my daily Aleve.
Next, an osteoporosis specialist recommended an infusion of the drug ReClast (zoledronic acid) but said that, with Medicare insurance, I could pay less if I had symptoms of GERD (acid reflux). Checking drug discount sites, I found conflicting information, with discounted prices from around $50 to more than $1,000. (A friend with different insurance took her ReClast prescription to CVS but only after many phone calls to her doctor and CVS could she coordinate getting the infusion to CVS and then scheduling it.) My specialist’s assistant was unfamiliar with pricing options but told me she had arranged for the hospital infusion technicians to call me. After more than four months I still have not gotten the infusion, and it appears I’m expected to research pricing myself.
I am least hopeful about overactive bladder medication for my wake-to-pee nocturia—a different form of overactive bladder than S.G. has —which, it turns out, does not respond well to tolterodine. The alternative, which operates via different receptors, could be helpful—but at what cost?
So, I’m dragging my feet, thinking I can live with the nighttime issues. Because I don’t have true osteoporosis but rather osteopenia, plus some other risk factors, maybe that drug is not urgent. Mostly, though, I’m aghast that anyone needs to go through such hoops to buy medication when they need it desperately and right away.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
MyLittleBird often includes links to products we write about. Our editorial choices are made independently; nonetheless, a purchase made through such a link can sometimes result in MyLittleBird receiving a commission on the sale, whether through a retailer, an online store or Amazon.com.
“LOOK AT at the label of your blush, face powder or eye shadow and you’ll likely see talc listed as an ingredient,” notes drugwatch. Other possible talc-containing products include mascara, concealer and moisturizers. Noting that the FDA considers talc GRAS (generally recognized as safe) in cosmetics, the site states: “Face powders often contain up to 100 percent talc, according to a safety report from the Cosmetic Ingredient Review Expert Panel. Other products, such as aerosol makeup bases, can be up to 35 percent talc.”
“Cosmetics is probably the best example of weak regulatory action leaving the American people unprotected,” former head of the Occupational Safety and Health Administration David Michaels told New Yorker writer Casey Cep. In her article “Damages,” Cep focuses on Johnson & Johnson’s sales of talc products—including those with traces of asbestos, “among the world’s deadliest carcinogens”—decades after documentation of the products’ health risks, notably of ovarian cancer.
Cosmetic companies—for whom only voluntary self-testing for ingredients is required—have claimed talc products made after 1976 to be “asbestos-free,” according to Cep. But “as recently as 2019 the FDA found asbestos in several talc products on store shelves—including in one bottle of J&J Baby Powder [which the company blamed on] testing error or contamination.”
And “studies that exposed lab animals to asbestos-free talc in various ways have had mixed results, with some showing tumor formation and others not finding any,” according to the American Cancer Society (ACS). Meanwhile,“talc that has asbestos is generally accepted as being able to cause cancer if it is inhaled.”
“The FDA’s Division of Cosmetics has “just 30 employees and an annual budget of less than ten million dollars…a twentieth of what it spends regulating food and drugs for pets,” writes Cep. “Whereas some countries’ regulators have banned more than 2,400 cosmetic ingredients, from parabens to formaldehyde, the FDA has banned or restricted fewer than a dozen.” According to Scott Faber at the Environmental Working Group (EWG), regulations covering “cosmetics,” including toothpaste, deodorant and shampoo, “are some of our most broken laws.”
“Independent testing has found hundreds of popular personal care items in the US to be contaminated with benzene,” according to the Guardian. Analyses have found benzene, a chemical linked to leukemia and other cancers, in everything from hand sanitizers to antiperspirants, lip products and moisturizers—“even if it’s not listed as an ingredient [and] most frequently in aerosol or spray products, some at levels the FDA has characterized as ‘life-threatening.’”
“Since 2009, 595 cosmetics manufacturers have reported using 88 chemicals in more than 73,000 products that have been linked to…serious health problems including cancer,” according to the EWG. And of “The Toxic Twelve Chemicals and Contaminants in Cosmetics” on the EWG’s latest list, the EU has banned every one of them.
Many of the “toxic twelve” have been slated for removal from store brands, according to a 2020 EWG report. In the report’s comparison of CVS Health with Whole Foods, CVS as of the end of 2019 prohibited the use of formaldehyde and substances known as PFAS that have been linked to cancer as well as hormone disrupting phthalates and parabens—but only “some of these are already banned from products sold in Whole Foods.”
Cosmetic chemicals enter the body through skin, inhalation, ingestion and internal use, but FDA authorization, while it ensures protection from harmful ingredients in food, does not extend to cosmetics. In addition, the FDA allows the omission from product labels of any chemical deemed a component of fragrance —a list that includes two phthalates, one of which has been classified as “possibly carcinogenic,” according to the EWG.
“No significant link” between women’s use of talcum powder on the genitals and cancer was the conclusion of a study published in JAMA of more than 250,000 women between 1976 and 2017. But the study authors noted that, even in the absence of asbestos, the powder could “induce an inflammatory response…could set off a cascade of increased oxidative stress levels…all of which could contribute to carcinogenesis.”
Baby powder using the mineral talc made its debut in J&J’s 1902 at-home birth kits. Cep describes a 1971 study analyzing tissue of reproductive-cancer patients that found “most of their cervical and ovarian tumors had talc in them.” Explains the ACS site: asbestos-free talc “might cause cancer in the ovaries” when applied to the genital area or on diaphragms or condoms—if the particles “were to travel through the vagina, uterus, and fallopian tubes to the ovary.”
“Johnson & Johnson has always insisted that its baby powder was ‘safe, asbestos-free and does not cause cancer,’” according to Cep. But in the past 20 years, a lethal form of cancer associated with asbestos exposure in men who worked in mining or construction, called mesothelioma, has shown up in “a much younger population and more women.” Now facing over 40,000 lawsuits in the US alleging that baby powder contaminated with asbestos caused ovarian cancer or mesothelioma, J&J has announced that after 2023, its baby powder will no longer contain talc, using cornstarch in its place.
Pulmonary fibrosis is another disease mentioned in connection with talc. In a 1969 memo, a J&J company scientist warned about “the possibility of adverse effects on the lungs of babies or mothers” and noted that “pulmonary fibrosis…might be rightfully or wrongfully attributed to inhalation of our power formulations.” According to a summary by Spanish researchers, “Over the last decades…the prevalence and incidence of IPF (idiopathic pulmonary fibrosis) have appeared to be increasing.”
Both my grandmother and father died after long bouts of lung disease, and my father’s diagnosis was pulmonary fibrosis. Reading about J&J’s introduction of baby powder in 1902 made me wonder whether sprinklings of talc on my father as a baby in the 1920s or the clouds of Chloe powder— with talc listed as an ingredient — that proceeded my grandmother everywhere played a role in their deaths.
I rarely used cosmetic products after several intense allergic reactions—notably to a Clinique facial that caused my eyes to swell shut for the remainder of the day. But I have used blush powder and other items containing talc. And we may, all of us who lived during the 20th century, have had frequent exposure to asbestos—infiltrating our daily lives in cement and building insulation, car parts and various home appliances.
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.
WHEN Hilary Mantel died last week, stroke was the immediate cause, but obituaries noted her long, painful history of endometriosis from about age 11 until a hysterectomy in her late 20s. “Endometriosis is what used to be called a female complaint…menstruation run amok,” writes Judith Shulevitz in the Atlantic. “The cells in the lining of the womb that usually bleed out during a period instead grow in other parts of the body.”
Endometriosis arises rarely in postmenopausal women—occurring in only 2 to 5% of those with the condition. Symptoms —digestive complaints, such as constipation, as well as pelvic discomfort—can indicate a 2-3% likelihood of cancer, usually ovarian. But many women have signs of endometriosis without symptoms, and even the cause of the condition is uncertain. Other than as an ongoing condition, endometriosis in those over 65 is most often associated with excessive production of estrogen and with obesity.
Postmenopausal women still, however, need regular gynecological exams —which focus on the entire pelvis: the bladder and rectum, as well as the genital organs. Associated with decreased production of estrogen after menopause, GSM (genitourinary syndrome of menopause) includes recurrent UTIs (urinary tract infections) and UI (urinary incontinence), as well as genital dryness, burning and irritation.
The incidence of UTIs rises “dramatically” with age—occurring in from 15-20% of women aged 65-70. According to British and Polish researchers, “Lack of awareness of the association between recurrent UTIs and GSM may result in multiple unnecessary courses of antibiotic therapy…and altered patterns of antimicrobial drug resistance.”
“Wake to pee” (getting up during the night more than once or twice to pee), or nocturia, is one form of urinary incontinence, which is linked to overactive bladder syndrome (OAB). Another is “urge incontinence,” in which the sensation of needing badly to pee comes on suddenly and strongly. Both conditions have responded well to drug treatment that includes hormone therapy, such as topical vaginal estrogen.
Hormone replacement therapy (HRT) using systemic estrogen as well as estrogen plus progesterone have led to a “significant reduction in prevalence [of nocturia] and its associated bother,” according to Belgian researcher Kim Pauwaert. But Pauwaert believes the effects can “mainly be explained by an impact on sleep disorders and sleep quality” associated with menopause. HRT has also helped counter recurrent UTIs.
Stress incontinence (SUI), the most common type of UI, refers to involuntary loss of urine due to increased intra-abdominal pressure—notoriously in response to coughing, sneezing or laughing. But causes of SUI can include any upright movement, like walking—due to the impact and to weight bearing down on the abdomen—as opposed, for example, to swimming where there is no impact and no weight bearing down. Treatments include Botox injections into the bladder; medications that calm an overactive bladder; and a surgically implanted mesh sling.
But the simplest and usually first-line treatment is usually Kegel exercises that, by strengthening the pelvic floor, can relieve OAB symptoms associated with both kinds of incontinence. Kegel exercises involve squeezing and holding pelvic muscles in a way that both contracts and lifts for several seconds, followed by relaxing for several seconds and then repeating. For women, one suggestion is to picture a straw going into your vagina and contract muscles as if to draw something up the straw.
Alternatively, devices that simulate the exercises can help people who tend to do Kegels incorrectly or insufficiently. Vaginal electrical stimulation (VES), which involves placing thin wires inside the vagina—or in the rear for men—can work better than Kegels to both strengthen pelvic muscles and encourage growth of nerve cells that signal muscle contraction.
The EmSella Chair —sometimes called a “Kegel Throne” – is a vibrating chair “that essentially does Kegel exercises for you — 20,000 reps in a single 30-minute treatment, to be exact,” according to SHAPE. Using the chair in a doctor’s office or clinic costs around $300 per session, usually for six sessions. A similar, older and less costly method uses shots to deliver electrical stimulation—a recommended 30 minutes a day over the course of 12 weeks—that can build stronger pelvic floor muscles, although many patients report unsatisfactory results. Most stimulation methods are not covered by insurance.
Gynecological exams after menopause also check genital organs for cancer. Pap smear screening for cervical cancer, however, is no longer recommended for those over 65 who have had at least three consecutive negative Pap results and no history of advanced precancer diagnosis, according to the U.S. Preventive Services Task Force.
For my part, I haven’t visited a gynecologist since before the pandemic, believing I did not need ongoing checkups. I just made an appointment, both to have a pelvic exam and to discuss nocturia and possibilities for relief. I have tried practical suggestions like restricting liquids for hours before bedtime, however, and am aware that most drug treatments, including estrogen suppositories and sleep aids, have unwanted side effects.
But I should take inspiration from Hilary Mantel, who spent her life ravaged by endometriosis—first from the surgery that removed her womb and ovaries, along with parts of her bladder and bowel; then from unrelenting, debilitating pain due to migraines associated with the condition; and finally from the excessive weight gained as a result of ongoing hormone treatments.
But, writes Shulevitz, Hilary Mantel “worked her experience until it became the corporeal substrate of her fiction. Her magnum opus is made of blood and female bodies.”
—Mary Carpenter regularly reports on need-to-know topics in health and medicine.